


The Sechenov Medical Journal is a scientific and practical peer-reviewed journal, the official publication of Sechenov University.
The Journal has been published since 2010 with a frequency of 4 issues per year and is intended for the health professionals.
The journal is ranked at Level 1 on the Unified State List of Scientific Publications, also known as the 'White List'.
The Title is included in the Russian Science Citation Index (RSCI) collection, based on the Russian Index of Science Citation(RISC) database and is in the Scopus database.
Sechenov Medical Journal publishes original articles, reviews, and clinical cases, covering a wide range of issues in biomedical sciences, fundamental and clinical medicine and concerned with important clinical and basic research in the field of:
- cell biology,
- pathological physiology,
- internal diseases,
- obstetrics and gynaecology,
- oncology, surgery
- neurosurgery.
Publication time frames:
5 days - first decision (accept for review or reject the manuscript)
40 days - average duration of the review phase
99 days - from manuscript submission to publication (average)
20% - of all manuscripts submitted during the year were accepted for publication
Mass media state registration certificate PI № ФС77-78884 dated August 28, 2020, issued by the Federal Service for Supervision of Communications, Information Technology and Mass Media (Roskomnadzor).
Current issue
INTERNAL MEDICINE
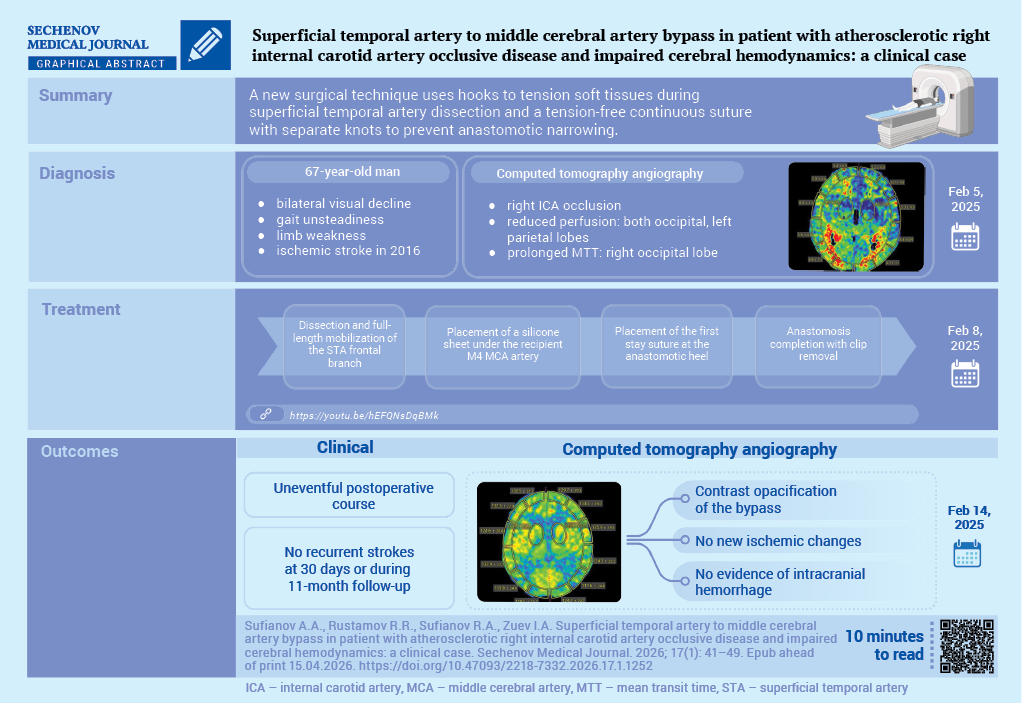
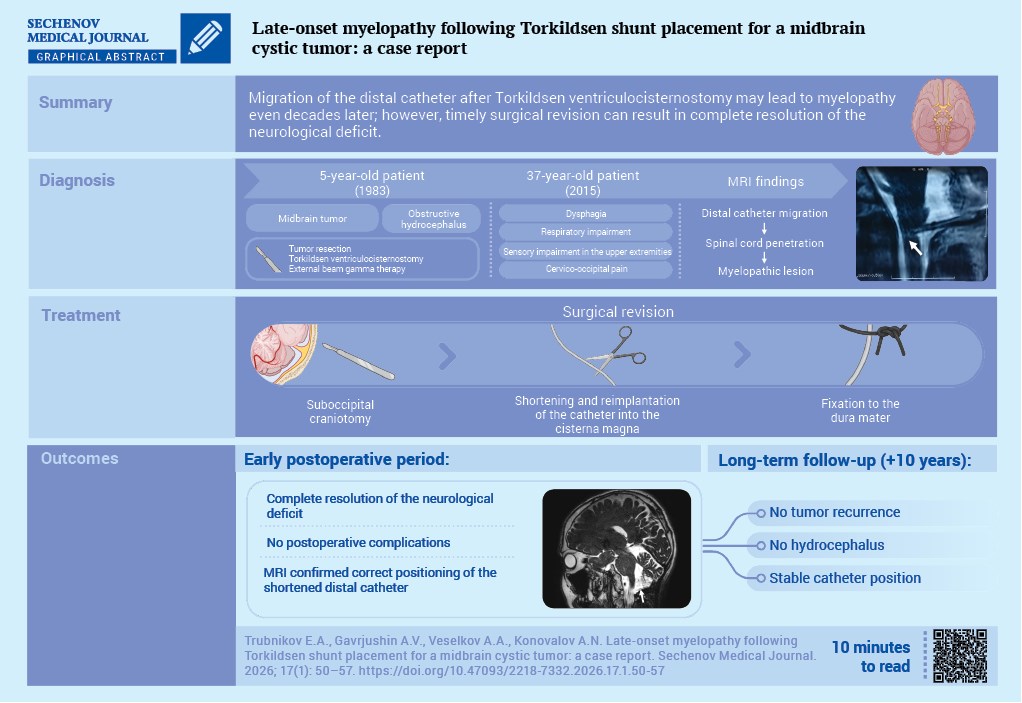
NEUROSURGERY
Announcements
2026-07-30
Special issue on Endovascular Surgery
Dear Colleagues,
We are pleased to inform you of a special issue of the Sechenov Medical Journal on Endovascular Surgery in 2026.
We will accept manuscripts formatted according to the journal's requirements until September 2026.
| More Announcements... |






















