




Contents
Scroll to:
https://doi.org/10.47093/2218-7332.2026.17.1.1252
Scroll to:
Cerebral revascularization by superficial temporal artery (STA) to middle cerebral artery (MCA) bypass is performed in patients with moyamoya disease, complex aneurysms, and selected extraand intracranial occlusive lesions to augment cerebral perfusion and potentially reduce the risk of ischemic complications and death.
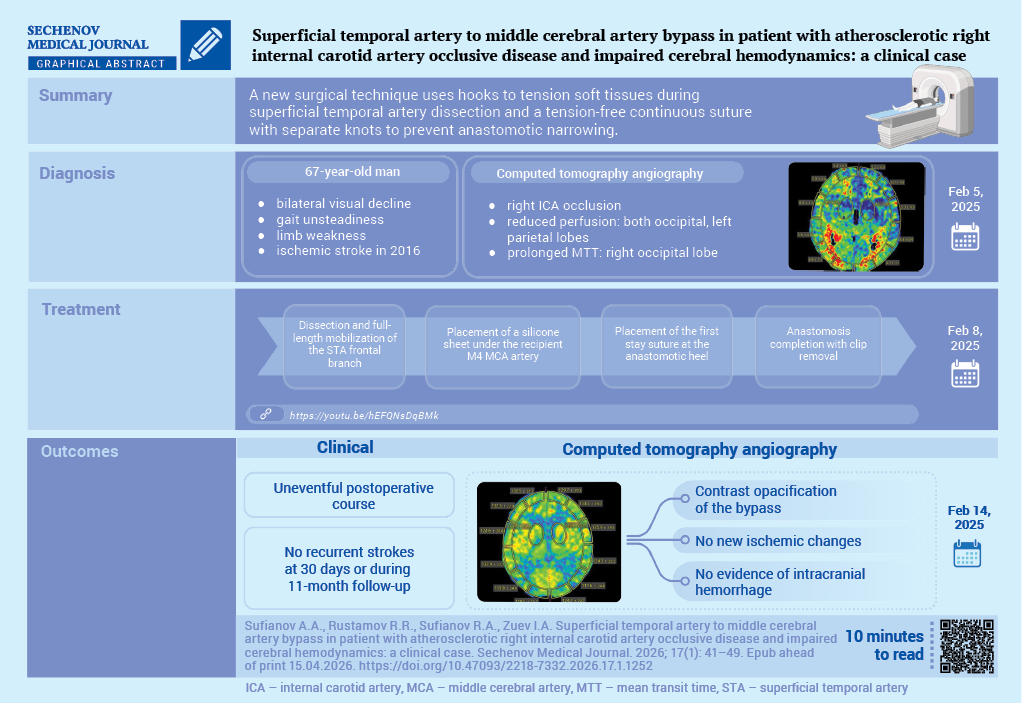
Case report. A 67-year-old patient presented with severe visual impairment (mainly on the right), gait unsteadiness, episodic subjective limb weakness, and marked fatigue. He had a significant medical history, having suffered an ischemic stroke in 2016 in the territory of the right MCA. A computed tomography angiography demonstrated occlusion of the right internal carotid artery and reduced cerebral blood flow in both occipital lobes and the left parietal lobe. An STA-MCA bypass anastomosis was performed. The postoperative course was uneventful; follow-up computed tomography angiography confirmed bypass patency without intracranial hemorrhage or new ischemic lesions, and a 10–15% increase in the cerebral blood volume index (up to 8.6 mL/100 g). No recurrent strokes were observed within 30 days and during 11 months of follow-up.
Discussion. Creation of an STA-MCA anastomosis may offer prospects for improving quality of life after ischemic stroke, including potential amelioration of post-stroke depression and other associated emotional disturbances.
Internal carotid artery (ICA) occlusion accounts for 15-20% of ischemic strokes and carries substantial risk of recurrent cerebrovascular events despite optimal medical management. Atherosclerotic ICA occlusion causes approximately 10% of transient ischemic attacks and 15% to 25% of ischemic strokes in the carotid territory [1–3]. The 2-year risk of subsequent ipsilateral ischemic stroke while a patient receives medical therapy is 10% to 15% [4]. While endovascular techniques address acute occlusions, chronic ICA occlusion remains resistant to recanalization, necessitating alternative revascularization approaches.
Extracranial-intracranial arterial bypass surgery was developed to prevent subsequent strokes by improving hemodynamics distal to the occluded artery [5][6]. In 1985, a randomized trial demonstrated no benefit of this surgery in 808 patients with symptomatic carotid artery occlusion [6–8]. This trial was criticized for failing to identify the subgroup of patients with hemodynamic cerebral ischemia due to poor collateral circulation for whom surgical revascularization might be of greatest benefit [3][5][9]. Contemporary neuroimaging, e.g. positron emission tomography, single photon emission computed tomography, computed tomography (CT) / magnetic resonance perfusion, enables precise identification of patients with hemodynamic cerebral ischemia. The Japanese extracranial-intracranial Bypass Trial and Carotid Occlusion Surgery Study demonstrated potential benefit in highly selected patients with severe hemodynamic compromise and increased oxygen extraction fraction, underscoring the importance of rigorous assessment and technical expertise [10][11].
The aim of this case report is to demonstrate the experience of superficial temporal artery (STA) to middle cerebral artery (MCA) bypass in a patient with atherosclerotic right ICA occlusive disease and impaired cerebral hemodynamics.
A 67-year-old man was admitted to the Cerebrovascular Pathology Department of Federal Center of Neurosurgery (Tyumen, Russia) on February 5, 2025, for evaluation of progressive bilateral visual loss (more on the right) and gait unsteadiness with staggering. He also reported intermittent subjective weakness in the arms and legs, generalized asthenia, and easy fatigability for a prolonged period. His medical history included an ischemic stroke in 2016 in the territory of the right MCA. Cardiovascular comorbidities comprised ischemic heart disease and atherosclerotic heart disease, post-infarction cardiosclerosis (since 2012), status post percutaneous transluminal coronary angioplasty with stent implantation, and stage III arterial hypertension.
On neurologic examination, consciousness was clear; memory was mildly reduced. Meningeal signs were absent. Cranial nerve assessment demonstrated marked bilateral visual impairment, more pronounced on the right. The range of motion in the limbs and trunk was preserved; muscle strength was symmetric (Medical Research Council grade 5/5 in both upper and lower extremities), despite episodic hand clumsiness (difficulty holding cutlery) and transient leg “weakness” by history. Sensory modalities were intact. Muscle tone was normal and symmetric (D=S). Deep tendon reflexes were brisk and symmetric in the upper and lower limbs; pathological reflexes were absent. He was unstable in the Romberg position. No clinically relevant abnormalities were detected on autonomic nervous system assessment; the somatic status was notable for generalized weakness and fatigue.
CT angiography of the brachiocephalic and cerebral arteries revealed occlusion of the right ICA (Fig. 1A). Brain CT perfusion demonstrated decreased cerebral blood flow and cerebral blood volume in both occipital lobes and in the left parietal lobe, together with prolonged mean transit time in the right occipital lobe (Fig. 1B–D).

FIG. 1. Computed tomography angiography of the brachiocephalic and cerebral arteries, February 5, 2025 (A), brain computed tomography perfusion, February 6, 2025 (B, C, D) before surgery.
A. Occlusion of the right internal carotid artery.
B. Decreased cerebral blood flow in the right occipital lobe.
C. Decreased cerebral blood volume in the right occipital lobe.
D. Increase mean transit time in the right occipital lobe.
Note: CCA – common carotid artery; ECA – external carotid artery; VA – vertebral artery.
The diagnosis was atherosclerosis of the brachiocephalic and cerebral arteries with occlusion of the right ICA; stenosis of the right common carotid artery up to 60% according to European Carotid Surgery Trial (ECST) criteria [11]; stenosis of the left ICA up to 30%; and 70% stenosis of the intracranial segment of the left ICA, complicated by vestibulo-ataxic syndrome.
The STA was marked preoperatively with Doppler ultrasonography. With the patient in the supine position, the head was rotated to the left and rigidly fixed in a Mayfield clamp. A skin incision was made along the course of the STA. The wound edges were retracted with skin hooks to optimize exposure. Layer-by-layer dissection of the subcutaneous tissue was performed over the course of the STA. The frontal branch was dissected and mobilized along its accessible length. Both frontal and parietal branches of the STA were isolated (Fig. 2A). A frontotemporal (dermofascial) flap was then elevated over the temporalis muscle. The temporalis fascia was incised, and the temporalis muscle was split and retracted to expose the calvarium.
A standard craniotomy was performed, and the dura mater was opened in a curvilinear fashion. Under the operating microscope, a cortical recipient vessel corresponding to the M4 segment of the right MCA was identified and sharply dissected from the arachnoid adhesions. The recipient artery was mobilized sufficiently to allow microsurgical manipulation, and a silicone background sheet was placed beneath the vessel (Fig. 2B).
The donor STA branch was prepared by gentle adventitial dissection and irrigation with heparinized saline. The distal end was trimmed in a fish-mouth configuration to match the arteriotomy. After systemic heparinization according to institutional protocol, temporary microvascular clips were applied proximally and distally on the recipient artery. The intended arteriotomy margins were marked, and a linear arteriotomy was performed.
An end-to-side STA–MCA anastomosis was constructed using standard microsurgical technique (Fig. 2C). Stay sutures were placed at the heel and tip to secure alignment and prevent torsion. The anastomosis was completed with sequential suturing along both vessel walls; in this case, a running technique with intermittent knot tying after division of the suture line was employed. Throughout the anastomosis, the field was continuously irrigated with heparinized saline to prevent desiccation of the intima and reduce the risk of thrombosis. The opposite wall was closed in a similar fashion, and the suture line was inspected for gaps and intimal inversion. A video of the operation is available at the link: https://youtu.be/hEFQNsDqBMk

FIG. 2. Bypass anastomosis of the superficial temporal artery to the middle cerebral artery.
A. Frontal branch of the superficial temporal artery was dissected and mobilized along its entire length.
B. A silicone background sheet was positioned beneath the recipient cortical artery.
C. Placement of the first stay suture at the heel of the anastomosis.
D. Completion of the anastomosis: final sutures placed, and temporary clips removed; intraoperative indocyanine green video-angiography confirmed bypass patency and flow.
Note: STA – superficial temporal artery.
Following completion, the temporary clips were removed to re-establish flow in the donor and recipient vessels. Intraoperative indocyanine green video-angiography confirmed immediate patency and antegrade flow through the bypass (Fig. 2D). Doppler ultrasonography further verified graft flow and anastomotic integrity (Fig. 3A–B). Postoperative CT angiography demonstrated contrast opacification of the bypass without evidence of intracranial hemorrhage or new ischemic changes. On follow-up imaging, perfusion assessment showed a moderate increase in the cerebral blood volume index by approximately 10–15%, reaching 8.6 mL/100 g (Fig. 3C–D).

FIG. 3. Postoperative computed tomography angiography (A, B) and computed tomography perfusion (C, D) obtained 6 days after surgery.
A. Coronal and axial reconstructions demonstrating contrast opacification of the superficial temporal artery–middle cerebral artery bypass microanastomosis (white arrows).
B. 3D reconstruction of the cerebral arteries without radiologic evidence of intracranial hematoma or acute ischemic changes.
C, D. Increased cerebral blood volume in the right occipital lobe.
In this case, the surgery was followed by an uneventful postoperative course with radiological confirmation of bypass patency on CT angiography and no evidence of intracranial hemorrhage or new ischemic lesions. Perfusion imaging performed on postoperative day 6 demonstrated a moderate increase in the cerebral blood volume index in the right occipital lobe. Although cerebral blood volume is an indirect surrogate of hemodynamic improvement and should be interpreted together with additional perfusion parameters, the observed direction of change is consistent with improved collateral supply after flow augmentation. Clinically, no recurrent strokes were observed within 30 days and during 11 months of follow-up which supports technical feasibility and short-to mid-term safety of the procedure in this highly selected patient with documented preoperative hemodynamic impairment.
The STA-MCA bypass technique developed by M.G. Yaşargil and R.M.P. Donaghy in the 1960s was rapidly adopted throughout the world as a procedure for surgical flow augmentation for ischemic cerebrovascular disease. The initial enthusiasm for revascularization in atherosclerotic cerebrovascular disease was substantially tempered by the landmark 1985 Extracranial-intracranial Bypass Study Group trial demonstrating failure to reduce stroke risk in 1377 patients with symptomatic disease [4]. Despite high graft patency and improved hemodynamic metrics, perioperative stroke and death rates in early trials were substantial, limiting net clinical benefit. Subsequently, the Carotid Occlusion Surgery Study reported by Powers et al. in 2011 attempted to identify patients with hemodynamic compromise through elevated oxygen extraction fraction on positron emission tomography imaging, but demonstrated no benefit of bypass over medical therapy with a 21% stroke rate at 2 years in the surgical group compared to 23% in medical therapy, complicated by 15% perioperative stroke rate [8–10].
In contrast, moyamoya disease has emerged as a clear indication for revascularization, with the Japan Adult Moyamoya Trial demonstrating that direct bypass prevents ischemic strokes and may reduce hemorrhagic risk by offloading hemodynamic stress from fragile moyamoya vessels [12]. Another established indication is flow preservation when planned vessel sacrifice is necessary for complex aneurysms or skull base tumors, though balloon test occlusion has limitations with approximately 3.7% ischemic events occurring despite passing BTO [2][4][10][11][13].
Technical approaches of bypass surgery are divided into low-flow and high-flow constructs. STA-MCA anastomosis remains the most widely employed low-flow technique, providing flows of 30–50 mL/min through end-to-side anastomosis using 10-0 or 11-0 microsutures with temporary recipient vessel occlusion for 25–40 minutes [3][6]. The number of research articles reassessing bypass surgery with appropriate indications and high quality of care has recently increased, and carotid artery and MCA occlusion surgery studies designed with careful consideration for several criticisms against Carotid Occlusion Surgery Study are now being conducted in many countries [10][13].
This case illustrates the technical feasibility of an STA-MCA bypass in a patient with chronic carotid occlusion and documented hemodynamic impairment. This procedure may offer potential quality-of-life benefits after stroke, including improvement of post-stroke depressive symptoms and other emotional disturbances, although such outcomes require systematic assessment. We demonstrate a modified technique for STA dissection using hooks to achieve adequate soft-tissue tension. In addition, a continuous suturing along one edge without tension combined with individually tied knots may help prevent anastomotic narrowing. Collectively, these technical nuances may facilitate STA–MCA bypass construction, enhance surgeon confidence, and potentially reduce procedure-related complications.
Albert A. Sufianov performed the surgical procedure described in the submitted publication, made a major contribution to its conception and design, and supervised the writing and editing of the scientific article. Rakhmonzhon R. Rustamov, Rinat A. Sufianov and Ilya A. Zuev contributed to the conception and design of the publication, prepared materials, wrote and edited the text, and created the illustrations and video. All authors approved the final version of the article and take responsibility for all aspects of the submitted work.
Compliance with ethical standards. Consent statement. The patient consented to the publication of the article “Superficial temporal artery to middle cerebral artery bypass in patient with atherosclerotic right internal carotid artery occlusive disease and impaired cerebral hemodynamics: a clinical case” in the “Sechenov Medical Journal”.
Conflict of interest. Albert A. Sufianov is a member of the editorial board and did not participate in the editorial review or decision-making on this article. Rakhmonzhon R. Rustamov, Rinat A. Sufianov, Ilya A. Zuev declare that there is no conflict of interest.
Financing. The study had no sponsorship (own resources).
Use of artificial intelligence. No artificial intelligence tools were used in the preparation of this manuscript.
1. Lukyanchikov V.A., Orlov E.A., Oganesyan M.V., et al. Anatomical bases of brain revascularization: choosing an extra-intracranial bypass option. Zh Vopr Neirokhir im. N. N. Burdenko. 2021; 85(6): 120–126 (In Russ.) https://doi.org/10.17116/neiro202185061120. PMID: 34951769
2. Wessels L., Hecht N., Vajkoczy P. Bypass in neurosurgery-indications and techniques. Neurosurg Rev. 2019 Jun; 42(2): 389–393. https://doi.org/10.1007/s10143-018-0966-9. Epub 2018 Mar 13. PMID: 29536207
3. Takizawa K. [Kamiyama-style STA-MCA bypass surgery]. No Shinkei Geka. 2022 Jul; 50(4): 759–766. Japanese. https://doi.org/10.11477/mf.1436204618. PMID: 35946364
4. Powers W.J., Clarke W.R., Grubb R.L. Jr., et al. Extracranial-intracranial bypass surgery for stroke prevention in hemodynamic cerebral ischemia: the Carotid Occlusion Surgery Study randomized trial. JAMA. 2011; 306(18): 1983–1992. https://doi.org/10.1001/jama.2011.1610. Erratum in: JAMA. 2011 Dec; 306(24): 2672. Obviagele, Bruce [corrected to Ovbiagele, Bruce]. PMID: 22068990
5. Rodríguez-Hernández A., Josephson S.A., Lawton M.T. Bypass surgery for the prevention of ischemic stroke: current indications and techniques. Neurocirugia (Astur). 2012 Feb; 23(1): 5–14. https://doi.org/10.1016/j.neucir.2011.11.001. PMID: 22520098
6. Yoshida K. [Evidence of STA-MCA Bypass-History and Overseas Articles]. No Shinkei Geka. 2022; 50(4): 735–744. https://doi.org/10.11477/mf.1436204615. PMID: 35946361
7. Sekhar L.N., Natarajan S.K., Ellenbogen R.G., Ghodke B. Cerebral revascularization for ischemia, aneurysms, and cranial base tumors. Neurosurgery. 2008; 62(6 Suppl 3): 1373–1408. https://doi.org/10.1227/01.neu.0000333803.97703.c6. PMID: 18695558
8. Thines L., Durand A., Penchet G., et al. Microsurgical neurovascular anastomosis: the example of superficial temporal artery to middle cerebral artery bypass. Technical principles. Neurochirurgie. 2014; 60(4): 158–164. https://doi.org/10.1016/j.neuchi.2014.03.004. Epub 2014 May 21. PMID: 24856046
9. Nomura M., Tamase A., Kamide T., et al. Superficial temporal artery-middle cerebral artery bypass using a thick STA after endarterectomy: a rescue technique. J Neurol Surg A Cent Eur Neurosurg. 2017; 78(6): 595–600. https://doi.org/10.1055/s-0037-1598050. Epub 2017 Jun 6. PMID: 28586938
10. Fischer G., Senger S., Sharif S., Oertel J. Superficial temporal artery to middle cerebral artery bypass via a minimized approach: operative nuances and problem-solving aspects. World Neurosurg. 2016 Apr; 88: 97–103. https://doi.org/10.1016/j.wneu.2015.12.029. Epub 2015 Dec 28. PMID: 26732960
11. Bonati L.H., Kakkos S., Berkefeld J., et al. European Stroke Organisation guideline on endarterectomy and stenting for carotid artery stenosis. Eur Stroke J. 2021 Jun; 6(2): I–XLVII. https://doi.org/10.1177/23969873211012121. Epub 2021 May 11. PMID: 34414302
12. Miyamoto S., Yoshimoto T., Hashimoto N., et al. Effects of extracranial-intracranial bypass for patients with hemorrhagic moyamoya disease: results of the Japan Adult Moyamoya Trial. Stroke. 2014 May; 45(5): 1415–1421. https://doi.org/10.1161/STROKEAHA.113.004386. Epub 2014 Mar 25. PMID: 24668203
13. The EC/IC Bypass Study Group. Failure of extracranial-intracranial arterial bypass to reduce the risk of ischemic stroke: results of an international randomized trial. N Engl J Med. 1985; 313(19): 1191–1200. https://doi.org/10.1056/NEJM198511073131904. PMID: 2865674
Albert A. Sufianov - Dr. of Sci. (Medicine), Professor, Corresponding Member of RAS, Chief Physician, Federal Center of Neurosurgery (Tyumen); Head of the Department of Neurosurgery, Petrovsky National Research Center of Surgery; Director, Educational and Scientific Institute of Neurosurgery, PFU.
5, 4th km Chervishevskogo trakta, Tyumen, 625032; 2, Abrikosovsky lane, Moscow, 119435; 6, Miklukho-Maklaya str., Moscow, 117198
Rakhmonzhon R. Rustamov - Cand. of Sci. (Medicine), Head of the Cerebrovascular Pathology Department (Neurosurgical Department No. 2), Federal Center of Neurosurgery (Tyumen); Assistant Professor, Department of Neurosurgery, Petrovsky National Research Center of Surgery.
5, 4th km Chervishevskogo trakta, Tyumen, 625032; 2, Abrikosovsky lane, Moscow, 119435
Rinat A. Sufianov - Cand. of Sci. (Medicine), Associate Professor, Department of Neurosurgery, Petrovsky National Research Center of Surgery; neurosurgeon, Federal Center of Neurosurgery (Tyumen).
5, 4th km Chervishevskogo trakta, Tyumen, 625032; 2, Abrikosovsky lane, Moscow, 119435
Ilya A. Zuev - neurosurgeon, Cerebrovascular Pathology Department (Neurosurgical Department No. 2), Federal Center of Neurosurgery (Tyumen).
5, 4th km Chervishevskogo trakta, Tyumen, 625032

|
1. CARE Checklist: for writing a case report | |
| Subject | ||
| Type | Исследовательские инструменты | |
Download
(540KB)
|
Indexing metadata ▾ | |
Sechenov Medical Journal. Editor's checklist for this article you can find here.
Название / Title | Обходной анастомоз поверхностной височной артерии к средней мозговой артерии при атеросклеротической окклюзии правой внутренней сонной артерии с нарушением церебральной гемодинамики: клинический случай/ Superficial temporal artery to middle cerebral artery bypass in patient with atherosclerotic right internal carotid arteryocclusive disease and impaired cerebral hemodynamics: a clinical case |
Раздел / Section
| НЕЙРОХИРУРГИЯ/ NEUROSURGERY
|
Тип / Article | Клинический случай / Сlinical case |
Номер / Number | 1252
|
Страна/территория / Country/Territory of origin | Россия / Russia |
Язык / Language | Английский / English
|
Источник / Manuscript source | Инициативная рукопись / Unsolicited manuscript |
Дата поступления / Received | 21.09.2025 |
Тип рецензирования / Type ofpeer-review | Двойное слепое / Double blind |
Язык рецензирования / Peer-review language | Английский / English
|
РЕЦЕНЗЕНТ А / REVIEWER A
Инициалы / Initials | 1252_А
|
Научная степень / Scientific degree | Доктор медицинских наук / PhD |
Страна/территория / Country/Territory | Япония / Japan
|
Дата рецензирования / Date of peer-review | 02.11.2026 |
Число раундов рецензирования / Number of peer-review rounds | 1 |
Финальное решение / Final decision | Принять к публикации / accept for publication
|
ПЕРВЫЙ РАУНД РЕЦЕНЗИРОВАНИЯ / FIRST ROUND OF PEER-REVIEW
Scientific quality: Grade A: Excellent
Language quality: Grade А: Priority publishing
Congratulations on your excellent surgery STA-MCA anastomosis for the patient with atherosclerotic ICA occlusion. I totally agree to the indication of this bypass procedure for not only to moyamoya patients but also the patient with atherosclerotic hemodynamically compromised status. The entire techniques were all accurate, meticulous to manage such small vessels, STA and M4. This video is educative for all Neurosurgeon and deserves to be published to SMJ.
CONCLUSION: accept for publication.
РЕЦЕНЗЕНТ B / REVIEWER B
Инициалы / Initials | 1252_В
|
Научная степень / Scientific degree | Доктор медицинских наук / Dr. of Sci. (Medicine)
|
Страна/территория / Country/Territory | Россия / Russia
|
Дата рецензирования / Date of peer-review | 23.11.25 |
Число раундов рецензирования / Number of peer-review rounds | 1 |
Финальное решение / Final decision | Принять к публикации / accept for publication |
ПЕРВЫЙ РАУНД РЕЦЕНЗИРОВАНИЯ / FIRST ROUND OF PEER-REVIEW
Scientific quality: Grade A: Excellent
Language quality: Grade А: Priority publishing
Surgical treatment of internal carotid artery lesions, particularly occlusive forms, is an extremely pressing issue, as these lesions indicate an advanced stage of the disease, often accompanied by severe neurological deficits, disability, and enormous direct and indirect socioeconomic costs associated with treatment expenses.
Although surgical methods for treating internal carotid artery (ICA) lesions encompass a wide range of procedures—including microsurgical and endovascular techniques—these are associated with a high risk of complications and are primarily used to treat large and giant cerebral aneurysms, traumatic and spontaneous carotid cavernous sinuses, Moyamoya disease and Takayasu’s arteritis, and complex skull base tumors, the creation of an alternative route for blood outflow to bypass the affected vascular segment by forming an extra-intracranial anastomosis for the treatment of occlusive cerebrovascular disease is of great interest.
It is noteworthy that there are few publications in both domestic and international literature describing cases of treatment for stenotic and occlusive, embolically dangerous stenoses of the internal carotid artery through the creation of a microsurgical bypass anastomosis, when the options for endovascular and other types of surgical interventions have been exhausted due to high risk, anatomical features of the vessels, or contraindications for dual antiplatelet therapy.
Thus, the presented clinical case with intraoperative video footage clearly demonstrates the feasibility of microsurgical cerebral revascularization with good treatment outcomes for types of cerebrovascular pathology that previously could not be radically cured or were considered inoperable, and it merits publication in a leading scientific journal.
CONCLUSION: accept for publication.
РЕЦЕНЗЕНТ C / REVIEWER C
Инициалы / Initials | 1252_А
|
Научная степень / Scientific degree | Доктор медицинских наук / PhD |
Страна/территория / Country/Territory | Чили / Chile
|
Дата рецензирования / Date of peer-review | 17.12.2026 |
Число раундов рецензирования / Number of peer-review rounds | 1 |
Финальное решение / Final decision | Принять к публикации / accept for publication
|
ПЕРВЫЙ РАУНД РЕЦЕНЗИРОВАНИЯ / FIRST ROUND OF PEER-REVIEW
Scientific quality: Grade A: Excellent
Language quality: Grade А: Priority publishing
Outstanding quality of the clinical case material. Congratulations!
CONCLUSION: accept for publication.
РЕКОМЕНДАЦИИ НАУЧНЫХ РЕДАКТОРОВ ЖУРНАЛА / RECOMMENDATIONS
OF THE SCIENTIFIC EDITORS OF THE JOURNAL
ПЕРВЫЙ РАУНД РЕЦЕНЗИРОВАНИЯ / FIRST ROUND OF PEER-REVIEW
The manuscript presents a technically demanding and clinically relevant video case report of a superficial temporal artery-middle cerebral artery (STA–MCA) bypass in a patient with atherosclerotic occlusion of the right internal carotid artery and impaired cerebral hemodynamics. The topic is fully aligned with the scope of the journal and will be of interest to cerebrovascular neurosurgeons and clinicians involved in surgical cerebral revascularization. The case is well chosen, illustrates decision making in a complex hemodynamic scenario, and has clear educational potential in terms of operative technique and perioperative imaging.
However, the manuscript requires substantive scientific and editorial refinement to meet the standards of a print article accompanying a video.
1) The manuscript should be clearly positioned as a case report with an associated surgical video, with standardized bilingual title, article type, section heading (“Neurosurgery / Video case report”), and affiliations harmonized between the Russian and English versions. The abstract must be expanded into a conventional structured summary (background, case description, main findings and postoperative course, conclusions) that is self-sufficient and does not rely on the video narration.
2) Keywords and MeSH terms should be aligned with the actual focus of the article (cerebral revascularization, STA–MCA bypass, ischemic stroke, internal carotid artery occlusion, cerebral blood volume) and kept consistent across both language versions.
3) The main text in its current form largely reproduces the video commentary and therefore needs to be reshaped into an autonomous case report with a clear narrative structure. It is recommended to organize the manuscript into the following sections: Introduction, Case description, Surgical technique, Postoperative course and follow up, Discussion, and Conclusion.
4) The case description should provide a more comprehensive clinical picture, including cardiovascular comorbidities, neurological status, detailed CT angiography and perfusion findings, and explicit justification for choosing STA–MCA bypass in the context of chronic right ICA occlusion and bilateral hemodynamic impairment.
5) The surgical technique should be described as a coherent sequence of key steps rather than as a time coded transcript, emphasizing the specific technical nuances that make the procedure educationally valuable (preoperative STA mapping, modified STA dissection using hooks, recipient vessel preparation, “fish mouth” configuration of the donor, suture strategy to prevent anastomotic narrowing, intraoperative indocyanine green angiography and Doppler verification).
6) The results and postoperative course should be presented in a dedicated section, summarizing imaging outcomes (bypass patency, absence of hemorrhage or new ischemia, quantitative change in cerebral blood volume), clinical evolution, and duration of follow up without recurrent stroke. This will allow readers to evaluate both technical success and short to midterm safety and effectiveness.
7) The discussion should be expanded beyond a descriptive commentary and integrated with the current evidence base on extracranial–intracranial bypass surgery. It is advisable to briefly review historical EC/IC bypass trials, contemporary data identifying subgroups with hemodynamic compromise who may benefit from surgery, and the place of STA–MCA bypass among low flow and high flow revascularization strategies. The presented case should be explicitly positioned within this context, highlighting indications, patient selection, and the rationale for the chosen technique.
CONCLUSION: major revision
ВТОРОЙ РАУНД РЕЦЕНЗИРОВАНИЯ / SECOND ROUND OF PEER-REVIEW
The revised manuscript adequately addresses the concerns raised during the initial review and now meets the scientific and editorial standards of the journal. The authors have substantially strengthened the narrative structure, transforming the submission from a video transcript into a fully developed, autonomous case report that can be read and cited independently of the video. The clinical description, imaging data, and operative details are now presented in a clear, coherent manner that will be informative for neurosurgeons and other specialists involved in cerebral revascularization.
The abstract has been expanded and structured, with a concise summary of the clinical context, case characteristics, key procedural aspects, and postoperative outcomes. Keywords and MeSH terms have been aligned with the actual focus of the article, and the bilingual metadata (title, affiliations, contact information, ethics, conflict of interest, funding, abbreviations, author contributions) have been harmonized according to journal style. The main text now follows a logical sequence (Introduction, Case report, Surgical technique, Postoperative course, Discussion, Conclusion), with sufficient clinical detail and clear justification of indications for STA–MCA bypass in the context of chronic carotid occlusion and documented hemodynamic impairment.
Importantly, the discussion has been significantly expanded and better integrated with the current literature on extracranial–intracranial bypass, carotid occlusion, and patient selection based on hemodynamic criteria. The authors position their case appropriately within this evidence base and highlight the educational value of the described technical nuances. The reference list has been updated and formatted to journal requirements, with relevant neurosurgical and cerebrovascular sources.
Considering these improvements, the manuscript is now suitable for publication as a video‑supported case report.
CONCLUSION: accept. The revised manuscript is approved for publication without further major changes.

8-2 Trubetskaya st., Moscow, 119048
Federal State Autonomous Educational Institution of Нigher Education I.M.Sechenov First Moscow State Medical University of the Ministry of Health of the Russian Federation (Sechenovskiy University)
E-mail: sechenovmedj@staff.sechenov.ru
Processing of personal data
































