




Contents
Scroll to:
https://doi.org/10.47093/2218-7332.2026.17.1.50-57
Scroll to:
Torkildsen ventriculocisternostomy was historically one of the principal surgical treatments for obstructive hydrocephalus. However, nowadays it tends to be regarded mainly as a salvage procedure when standard shunting or endoscopic ventriculostomy is not feasible.
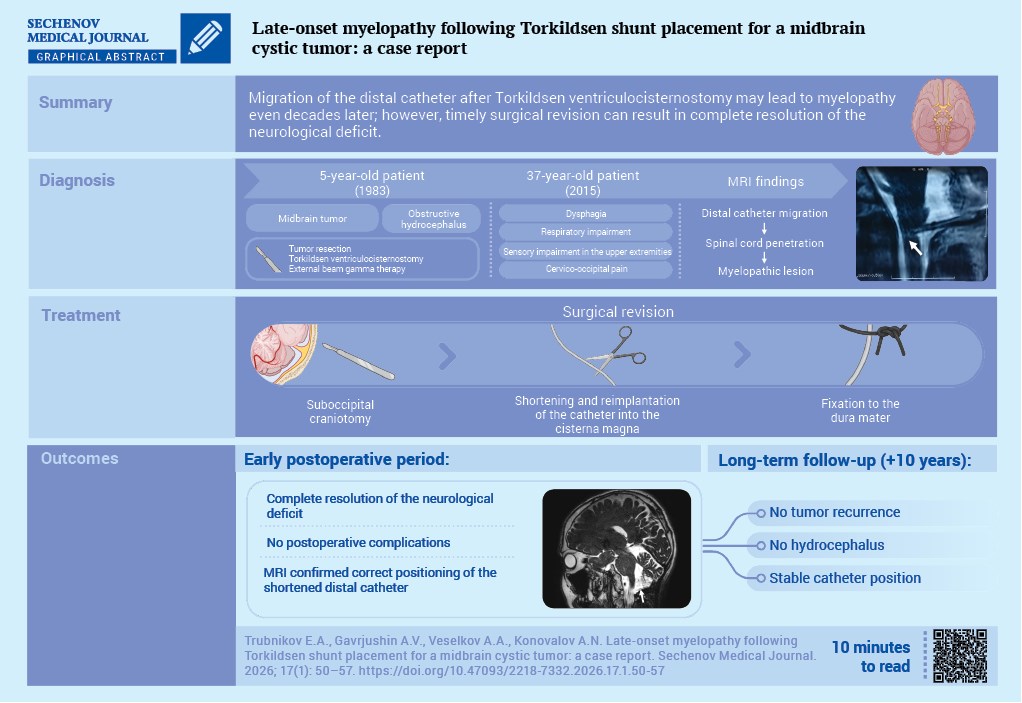
Case report. A 5-year-old boy with obstructive hydrocephalus secondary to a cystic midbrain tumor underwent tumor resection combined with Torkildsen ventriculocisternostomy. Postoperatively, adjuvant radiotherapy was administered, resulting in long-term disease stabilization. At the age of 37 years, 32–33 years after surgery, he developed dysphagia, respiratory disturbances, cervico-occipital pain, and sensory impairment in the upper limbs. Magnetic resonance imaging demonstrated migration of the distal catheter tip with penetration into the upper cervical spinal cord segments and formation of a focal myelopathic lesion. A suboccipital craniotomy was performed; the migrated catheter segment was removed, the system was shortened, and the distal end was reimplanted into the cisterna magna with fixation to the dura mater. Complete regression of neurological deficits was achieved, with a favorable 10-year follow-up.
Discussion. We report a rare delayed case of myelopathy caused by migration of the cisternal catheter tip more than 30 years after Torkildsen ventriculocisternostomy. This observation highlights the need for lifelong surveillance of patients who have undergone such procedures, strict adherence to surgical technique (appropriate catheter length selection and secure fixation), and timely surgical revision at the earliest signs of brainstem dysfunction or involvement of the upper cervical spinal cord.
Torkildsen ventriculocisternostomy was historically one of the earliest and most widely used surgical procedures for the treatment of obstructive hydrocephalus. However, in contemporary neurosurgical practice it is regarded mainly as a rescue procedure [1]. Nevertheless, patients with functioning or modified Torkildsen shunt systems continue to be encountered in clinical practice, which underscores the importance of assessing long-term complications of these interventions [2].
Clinically significant late complications include migration of the distal catheter tip with penetration into surrounding structures, including the cervical spinal cord, resulting in myelopathy. Such cases are considered extremely rare but potentially disabling and often require revision surgery at the craniovertebral junction [3].
Despite various technical modifications and catheter fixation techniques, the risk of distal catheter dislocation and penetration into adjacent tissues cannot be completely eliminated [4]. In this context, isolated clinical observations with a very long interval after the primary operation are of particular interest for understanding the pathogenesis of these complications, refining revision strategies, and assessing long-term prognosis.
The aim of this report is to present a rare case of distal ventricular catheter migration into the upper cervical spinal cord occurring 33 years after surgery for a cystic midbrain tumor, and to analyze the results of catheter reimplantation together with long-term (10-year) follow-up outcomes.
Hydrocephalus first manifested in a 5-year-old boy as diplopia caused by alternating strabismus. His general somatic condition at admission was as expected for his age. A neurological examination revealed brainstem signs, including fine horizontal nystagmus on extreme gaze and static ataxia. Computed tomography demonstrated a midbrain mass with evidence of aqueductal obstruction at the level of the cerebral aqueduct.
The patient underwent surgery. Intraoperatively, a lesion with a predominantly cystic component was identified and resected. The limited amount of biopsy material did not permit histological verification of the lesion. To prevent recurrent hydrocephalus in the event of possible tumor regrowth, the procedure was supplemented with Torkildsen ventriculocisternostomy. The ventricular catheter length was selected according to the patient’s anthropometric characteristics. The catheter was secured to the dura mater with interrupted sutures at two points to ensure stable positioning.
Following treatment, the patient’s condition was satisfactory. Neurological examination demonstrated persistent mild brainstem signs at the level of the pontine tegmentum, including diplopia and fine horizontal nystagmus. In the postoperative period, a course of adjuvant external beam gamma therapy was administered (20 sessions), with a total focal dose of 40 Gy delivered to the operative field. During subsequent follow-up, the patient remained clinically stable, with no evidence of deterioration.
Clinical deterioration occurred at the age of 37 years. In September 2015, the patient presented with dysphagia, respiratory disturbances, and sensory loss in the upper extremities. These symptoms had been present for one month before admission and had progressively worsened.
General condition on admission was satisfactory. The patient was alert and oriented, with a Glasgow Coma Scale score of 15; respiratory rate was 17 breaths per minute, heart rate 75 beats per minute, and blood pressure 125/80 mmHg. Neurological examination, in addition to persistent brainstem signs (horizontal nystagmus), revealed impaired proprioceptive and kinesthetic sensation in the upper extremities, accompanied by localized pain in the cervico-occipital region.
Magnetic resonance imaging (MRI) showed no evidence of tumor recurrence but demonstrated migration of the distal ventricular catheter tip with penetration into the spinal cord at the spinomedullary junction (Fig. 1A, B).

FIG. 1. Preoperative magnetic resonance imaging data of a 37-year-old patient with dislocation of the distal ventricular catheter tip (September 23, 2015).
A. T2-weighted sagittal image demonstrating penetration of the distal shunt catheter tip into the spinal cord at the level of the upper cervical segments (arrow).
B. T2-FLAIR coronal image demonstrating a hyperintense lesion with ill-defined margins corresponding to focal myelopathy (arrow).
The development of neurological deficits associated with migration of the distal catheter tip into the upper cervical spinal cord and the presence of myelopathic lesions on MRI constituted an indication for revision surgery.
The operation was performed on September 30, 2015. A midline suboccipital craniotomy with bone flap replacement was carried out. In the region of the posterior median sulcus of the upper cervical spinal cord, the migrated catheter tip was identified embedded within the spinal cord parenchyma. After removal, the distal catheter segment was shortened and reimplanted into the cisterna magna; the distal end of the ventricular catheter was additionally secured to the dura mater. The postoperative course was uneventful, and the patient was discharged in satisfactory condition on postoperative day 5. At discharge, complete resolution of the neurological deficit was observed, with no new focal neurological signs.
One month after surgery, follow-up MRI confirmed correct positioning of the shortened distal ventricular catheter tip within the cisterna magna, with no evidence of tumor recurrence (Fig. 2A, B).

FIG. 2. Magnetic resonance imaging of the brain performed 1 month after surgery (October 29, 2015).
A. T2-weighted sagittal image showing the shortened distal ventricular catheter tip reimplanted into the cisterna magna (arrow).
B. T2-weighted sagittal image showing the proximal ventricular catheter segment in correct position (arrow); the middle third of the catheter courses through the occipital subgaleal space. No evidence of tumor recurrence is seen.
At the 10-year follow-up after ventricular catheter reimplantation, the patient reported only occasional cervico-occipital pain, with no focal neurological deficits. Annual follow-up MRI demonstrated no significant interval changes: there was no evidence of tumor progression or hydrocephalus, and the ventricular catheter remained in proper position.
In the present case, the total follow-up duration was 43 years, representing a rare and virtually unique experience in the management of a patient after Torkildsen ventriculocisternostomy. This highlights the fact that the long-term consequences of this procedure remain clinically relevant because despite the emergence of alternative extra- and intracranial shunting techniques, ventriculocisternostomy and its modifications continue to be used, albeit rarely, in modern neurosurgery [2][5].
During the first decades of Torkildsen ventriculocisternostomy use, a pooled analysis of 136 published cases by J.E. Scarff [6] showed that arrest of hydrocephalus progression over a two-year period was achieved in 58% of patients, with an operative mortality of approximately 30%. According to N. Morota et al. [7], these unfavorable outcomes in historical series largely reflect the level of neuroimaging, anesthetic, and neurosurgical care available in the mid-20th century, when the procedure was performed as a palliative intervention in severely ill, often terminal patients with advanced obstructive hydrocephalus. Nevertheless, the long-term effectiveness of the technique is supported by isolated case reports with follow-up periods of up to 30 and 50 years, demonstrating durable shunt function and satisfactory neurological outcomes [1][8].
Complications of Torkildsen ventriculocisternostomy include infectious and nonspecific surgical complications (wound infection, meningitis), mechanical shunt dysfunction (migration, kinking, axial rotation, and catheter obstruction), as well as neurological complications such as myelopathy, tetraparesis, and facial pain caused by penetration of the cisternal catheter tip into the brainstem or upper cervical spinal cord [3][7][9].
Myelopathy is considered one of the most serious, although rare, long-term complications of Torkildsen ventriculocisternostomy. It results from migration or progressive intraparenchymal advancement of the distal catheter tip, causing compression of the cervical spinal cord and craniocervical junction. Such cases have been reported both 8–15 years after surgery and as late as 25–30 years or more thereafter. Clinically, patients may present with progressive spastic tetraparesis, sensory disturbances, and signs of medullary involvement, whereas MRI can demonstrate the catheter penetrating the brainstem parenchyma or upper cervical spinal cord. Treatment usually consists of catheter removal, shortening, or repositioning with fixation to the dura mater; however, because of prolonged compression, neurological deficits often resolve only partially, underscoring the importance of early diagnosis and prevention of catheter migration [3][4][10][11].
In the present case, myelopathy developed 32 years after Torkildsen ventriculocisternostomy and was most likely related to inappropriate selection of ventricular catheter length and insufficient fixation to the dura mater, resulting in gradual distal catheter migration with penetration into the brainstem. Surgical correction consisted of revision of the shunt system, removal of the migrated catheter segment, shortening and reimplantation of the cisternal end, and additional fixation to the dura mater.
To prevent myelopathy caused by migration or excessive advancement of the cisternal catheter tip, G. Ehni et al. [3] emphasized the need for careful selection of catheter length according to the patient’s age, so that the catheter lies closely along the bone and enters the subarachnoid space of the cisterna magna only minimally. They additionally recommended positioning the distal tip strictly in the midline and securing it firmly to the dura and arachnoid mater with non-absorbable sutures, splitting the catheter tip into two thin “arms” to improve fixation. N. Morota et al. [7], based on their experience in pediatric patients, also highlighted the importance of thorough preoperative MRI assessment of the craniovertebral junction, partial resection of the posterior arch of the first cervical vertebra when necessary, and careful insertion of the catheter through a midline dural opening while limiting its intradural length to approximately 2 cm, thereby reducing the risk of compression of the brainstem and upper cervical spinal cord.
In the present case, the most likely cause of myelopathy was insufficient fixation of the ventricular catheter to the dura mater, which contributed to gradual distal catheter displacement with penetration into the brainstem. Timely diagnosis and surgical correction resulted in rapid and complete resolution of the neurological deficit.
Thus, the role of Torkildsen ventriculocisternostomy in contemporary neurosurgical practice remains debatable in the era of widespread use of endoscopic third ventriculostomy and various ventriculoperitoneal shunting techniques. In most patients, these methods are considered first-line treatment options, whereas the Torkildsen procedure and its modifications may serve as a salvage option in carefully selected cases of obstructive hydrocephalus where anatomical constraints or prior surgery limit the use of standard techniques. In such rare situations, strict adherence to technical principles – including optimal catheter length selection, secure fixation, and thoughtful revision of previously implanted shunt systems – may reduce the risk of severe complications and improve long-term clinical outcomes.
The present case demonstrates that Torkildsen ventriculocisternostomy may provide durable long-term control of obstructive hydrocephalus. However, sustained shunt function is associated with a risk of severe delayed complications related to the position of the cisternal catheter. The occurrence of myelopathy decades after surgery underscores the need for lifelong surveillance of patients who have undergone this type of cerebrospinal fluid shunting procedure, as well as timely system revision at the earliest signs of brainstem or cervical spinal cord involvement. Taken together, the available literature and the present case suggest that, in contemporary neurosurgery, the Torkildsen procedure should be regarded primarily as a reserve option for a limited subset of patients with obstructive hydrocephalus, whereas endoscopic third ventriculostomy and ventriculoperitoneal shunting remain the standard first-line treatments. In the rare situations in which ventriculocisternostomy is selected, meticulous surgical technique–including precise catheter length selection and secure fixation–is essential to reduce the risk of late complications and achieve favorable long-term outcomes.
Alexander N. Konovalov developed the concept. Elisey A. Trubnikov prepared the draft of the manuscript. Andrey V. Gavrjushin and Aleksei A. Veselkov contributed to the reviewing and editing of the text. Aleksei A. Veselkov and Elisey A. Trubnikov participated in data collection and patient examination. Andrey V. Gavrjushin performed the formal analysis. Alexander N. Konovalov was responsible for the methodology and provided scientific supervision throughout the study. All authors have approved the final version of the article.
Compliance with ethical standards. Consent statement. The patient consented to the publication of the article “Late-onset myelopathy following Torkildsen shunt placement for a midbrain cystic tumor: a case report” in the “Sechenov Medical Journal”.
Conflict of interest. The authors declare that there is no conflict of interest.
Financing. The study was unfunded (own resources).
Use of artificial intelligence. No artificial intelligence tools were used in the preparation of this manuscript.
1. Zinn P.O., Bozinov O., Burkhardt J.K., et al. Failure of a Torkildsen shunt after functioning for 50 years. J Neurosurg. 2010 Apr; 112(4): 796–799. https://doi.org/10.3171/2009.7.JNS09729. PMID: 19715420
2. Florian I.Ş., Aldea C.C. Ventriculocisternal shunt redivivus: third ventricle-cisterna magna intradural shunt: a technical note and case report. World Neurosurg. 2018 Aug; 116: 56–59. https://doi.org/10.1016/j.wneu.2018.05.034. Epub 2018 May 14. PMID: 29772362
3. Ehni G., Moiel R.H., Bragg T.G. Torkildsen's ventriculocisternostomy: some complications and their prevention. Clin Neurol Neurosurg. 1976; 79(2): 119–132. https://doi.org/10.1016/0303-8467(76)90004-4. PMID: 1029636
4. Crotty G.F., McKee K.E., Klufas R., et al. Progressive cervical myelopathy due to intramedullary migration of forgotten Torkildsen shunt. Neurology. 2019 Sep; 93(12): 555–556. https://doi.org/10.1212/WNL.0000000000008136. PMID: 31527098
5. Tang M., Richard S.A., Ren Y., et al. Aqueduct-fourth ventriclecisterna magna shunting as a prophylactic procedure for postoperative hydrocephalus in selective fourth ventricular tumors: A retrospective study. Medicine (Baltimore). 2025 Aug; 104(34): e43697. https://doi.org/10.1097/MD.0000000000043697. PMID: 40859526
6. Scarff J.E. Treatment of hydrocephalus: an historical and critical review of methods and results. J Neurol Neurosurg Psychiatry. 1963 Feb; 26(1): 1–26. https://doi.org/10.1136/jnnp.26.1.1. PMID: 13976518
7. Morota N., Ihara S., Araki T. Torkildsen shunt: re-evaluation of the historical procedure. Childs Nerv Syst. 2010 Dec; 26(12): 1705–1710. https://doi.org/10.1007/s00381-010-1182-2. Epub 2010 May 26. PMID: 20502902
8. Eide P.K., Lundar T. Arne Torkildsen and the ventriculocisternal shunt: the first clinically successful shunt for hydrocephalus. J Neurosurg. 2016 May; 124(5): 1421–1428. https://doi.org/10.3171/2015.1.JNS142659. Epub 2015 Sep 4. PMID: 26339852
9. Bervitskiy A.V., Moysak G.I., Dmitriev A.B., Rzaev D.A. Facial pain, caused by Torkildsen shunt migration. Russian journal of neurosurgery. 2020; 22(1): 71–76. (In Russian). https://doi.org/10.17650/1683-3295-2020-22-1-71-76. EDN: FPSECW
10. Schulder M., Maniker A.H., Lee H.J. Cervical myelopathy due to migration of Torkildsen's shunt: case report. Surg Neurol. 1999 Jan; 51(1): 27–30. https://doi.org/10.1016/s0090-3019(97)00433-3. PMID: 9952120
11. Pascual-Leone A., Dhuna A., Castillo R., Ala T. Displaced Torkildsen's shunt: an unusual cause of cervical myelopathy. J Neurol Neurosurg Psychiatry. 1991 Jul; 54(7): 654. https://doi.org/10.1136/jnnp.54.7.654. PMID: 1895134
Elisey A. Trubnikov - resident, 7th Neurosurgical Department (Glial Tumors).
16, 4th Tverskaya-Yamskaya str., Moscow, 125047
Andrey V. Gavrjushin - Cand. of Sci. (Medicine), research associate, neurosurgeon, 7th Neurosurgical Department (Glial Tumors).
16, 4th Tverskaya-Yamskaya str., Moscow, 125047
Aleksei A. Veselkov - neurosurgeon, 2nd Neurosurgical Department (Pediatric Neurosurgery).
16, 4th Tverskaya-Yamskaya str., Moscow, 125047
Alexander N. Konovalov - Dr. of Sci. (Medicine), Academician of the RAS, Professor, neurosurgeon, Honorary President.
16, 4th Tverskaya-Yamskaya str., Moscow, 125047

|
1. CARE Checklist | |
| Subject | ||
| Type | Research Instrument | |
Download
(499KB)
|
Indexing metadata ▾ | |
Sechenov Medical Journal. Editor's checklist for this article you can find here.
Название / Title | Миелопатия как отдаленное осложнение операции Торкильдсена у больного с кистозной опухолью среднего мозга: клиническое наблюдение / Late-onset myelopathy following Torkildsen shunt placement for a midbrain cystic tumor: a case report |
Раздел / Section
| НЕЙРОХИРУРГИЯ/ NEUROSURGERY
|
Тип / Article | Клинический случай / Сlinical case |
Номер / Number | 1435
|
Страна/территория / Country/Territory of origin | Россия / Russia |
Язык / Language | Русский / Russian Английский / English
|
Источник / Manuscript source | Инициативная рукопись / Unsolicited manuscript |
Дата поступления / Received | 17.01.2026 |
Тип рецензирования / Type ofpeer-review | Двойное слепое / Double blind |
Язык рецензирования / Peer-review language | Русский / Russian
|
РЕЦЕНЗЕНТ А / REVIEWER A
Инициалы / Initials | 1435_А
|
Научная степень / Scientific degree | Кандидат медицинских наук / Cand. of Sci. (Medicine) |
Страна/территория / Country/Territory | Россия / Russian
|
Дата рецензирования / Date of peer-review | 25.02.2026 |
Число раундов рецензирования / Number of peer-review rounds | 1 |
Финальное решение / Final decision | требуется незначительная доработка/ minor revision
|
ПЕРВЫЙ РАУНД РЕЦЕНЗИРОВАНИЯ / FIRST ROUND OF PEER-REVIEW
Актуальность статьи не вызывает сомнений. Статьи, посвященные анализу отдаленных осложнений оперативного лечения всегда представляют особый интерес.
До широкого внедрения в нейрохирургическую практику вентрикулоперитонеального шунтирования и эндоскопической триветрикулостомии, операция Торкильдсена (стент внутреннего дренирования) являлась одной из немногих возможностей сброса ликвора в обход блокированных вследствие различных причин ликворопроводящих путей. Миграция установленного стента встречалась у многих нейрохирургов, выполняющих эту операцию. По мере накопления опыта проведения операции пришло понимание важности правильного подбора длины стента, оптимального угла погружения стента в большую затылочную цистерну мозга и фиксации к ТМО большой затылочной цистерны. Использовали максимально пологую траекторию погружения стента в большую затылочную цистерну, длина стента различалась в зависимости от возраста пациента (у детей предусматривался «запас» длины с учетом дальнейшего роста организма), у взрослых обязательная «жесткая фиксация» места погружения в большую затылочную цистерну с использованием дополнительной муфты стента. В настоящее время операция Торкильдсена практически не используется, за исключением редких случаев паллиативных вмешательств, однако пациенты с ранее выполненными операциями попадают в поле зрения неврологов и нейрохирургов.
Из представленных материалов статьи предполагается, что операция была выполнена с оставлением «запаса длины» стента, с учетом дальнейшего роста оперированного ребенка. Не совсем ясно как именно фиксировался стент, или он был фиксирован только швом ТМО. Для лучшего понимания причин и времени возникновения осложнения хотелось бы привести выписку из протокола операции и данные КТ или МРТ сразу после операции или за прошедшие 33 года до развития осложнений.
На представленных постоперационных МРТ дистальный конец стента погружен в большую затылочную цистерну в верхних отделах и видимо только там фиксирован, что с учетом анатомических особенностей пациента приводит к позиции дистального конца практически перпендикулярно спинному мозгу, что потенциально может повторно привести к уже описанному осложнению.
Возможно следует изменить формулировку «Данное наблюдение демонстрирует уникальный случай развития миелопатии, которая не была связана с прогрессированием опухоли или дефектами первоначального хирургического вмешательства», так как это осложнение связано с неудачным позиционированием дистального конца стента в большой затылочной цистерне практически перпендикулярно спинному мозгу. При данной анатомической форме задней черепной ямки возможно позиционирование дистального конца с фиксацией к ТМО в двух местах на протяжении для сохранения направления стента.
Имеется несоответствие между утверждением об уникальности описываемого осложнения и приведением в списке литературы источника №6, где описана миелопатия как осложнение миграции стента.
Статья написана стилистически и грамматически верно. Литературные источники актуальны и соответствуют теме работы.
Имеющиеся недостатки не снижают оценку проведённой̆ работы.
ЗАКЛЮЧЕНИЕ: требуется незначительная доработка.
РЕЦЕНЗЕНТ B / REVIEWER B
Инициалы / Initials | 1435_В
|
Научная степень / Scientific degree | Кандидат медицинских наук / Cand. of Sci. (Medicine)
|
Страна/территория / Country/Territory | Россия / Russia
|
Дата рецензирования / Date of peer-review | 06.04.2026 |
Число раундов рецензирования / Number of peer-review rounds | 1 |
Финальное решение / Final decision | Принять к публикации / accept for publication |
ПЕРВЫЙ РАУНД РЕЦЕНЗИРОВАНИЯ / FIRST ROUND OF PEER-REVIEW
Представленная работа посвящена клиническому случаю операции вентрикулоцистерностомии по Торкильдсену и описанию осложнения через 33 года. Рукопись представляет явный интерес с клинической точки зрения отдаленных результатов операции и их коррекции. Но по содержанию есть небольшие замечания, которые нужно учесть.
В тексте содержится ошибка относительно даты первого выполнения операции. Авторы указывают, что первая операция была выполнена Торкильдсеном в 1939 году, и в источнике норвежского журнала тоже есть ошибка. Фактически операция проведена 9 сентября 1937 года, согласно оригинальной публикации Fincher E.F. et al. (1948). Fincher E.F., Strewler G.J., Swanson H.S. The Torkildsen Procedure: A Report of 19 Cases. Journal of Neurosurgery. 1948; 5(3): 213–229. DOI: 10.3171/jns.1948.5.3.0213
В разделе «Обсуждение» авторы прямо указывают: «По нашему мнению, потенциальными причинами развития осложнения в представленном наблюдении мог стать неправильный подбор длины вентрикулярного катетера с непрочной фиксацией к твердой мозговой оболочке». Таким образом, авторы фактически признают техническую ошибку при выполнении первичного вмешательства, что входит в противоречие с представлением случая как примера отдаленного осложнения, «не связанного с дефектами первоначального хирургического вмешательства» (аннотация). Необходимо однозначно определить позицию: либо это техническая ошибка при установке шунта, либо отдаленное осложнение правильно выполненной операции. Смешение этих концепций недопустимо.
Хотелось бы все-таки получить МРТ-изображения опухоли с внутривенным контрастным усилением до оперативного вмешательства, что не позволяет оценить обоснование выбора операции Торкильдсена в качестве метода ликворошунтирования; а также МРТ-данные ложа удаленной опухоли, необходимые для оценки радикальности резекции и послеоперационных изменений, структуры водопровода мозга.
В обсуждении нужно дополнить разными модификациями операции Torkildsen для профилактики таких осложнений, которые были и у других авторов.
Рукопись представляет интерес к публикации редкого случая, однако в представленном виде не может быть рекомендована к публикации. Требуется доработка с устранением фактологических ошибок, противоречий и дополнением клинического материала соответствующей визуализацией. После внесения указанных исправлений рукопись может быть направлена на повторное рецензирование.
ЗАКЛЮЧЕНИЕ: переработка и повторное рецензирование.
ВТОРОЙ РАУНД РЕЦЕНЗИРОВАНИЯ / SECOND ROUND OF PEER-REVIEW
Все замечания авторами учтены.
ЗАКЛЮЧЕНИЕ: принять к публикации.
РЕКОМЕНДАЦИИ НАУЧНЫХ РЕДАКТОРОВ ЖУРНАЛА / RECOMMENDATIONS
OF THE SCIENTIFIC EDITORS OF THE JOURNAL
ПЕРВЫЙ РАУНД РЕЦЕНЗИРОВАНИЯ / FIRST ROUND OF PEER-REVIEW
Рукопись посвящена редкому отдалённому осложнению вентрикулоцистерностомии по Торкильдсену с формированием миелопатии через 33 года после вмешательства, что представляет несомненный клинический интерес и может быть полезно практикующим нейрохирургам и неврологам. Хорошо структурированное клиническое описание, наличие длительного катамнеза (43 года) повышают ценность работы.
Вместе с тем, в текущем виде рукопись не полностью соответствует издательскому стандарту журнала.
Ключевые слова
Добавить 5-7 ключевых слов, слова не должны напрямую упоминаться в названии рукописи.
Ключевые положения
Добавить от 3 до 5 ключевых положений (не должны повторять заключение)
Аннотация
Оформить аннотацию по требованиям журнала.
Цель
Сформулировать цель описания данного случая.
Описание случая
Список литературы
Технические требования
ЗАКЛЮЧЕНИЕ: переработка и повторное рецензирование.
ВТОРОЙ РАУНД РЕЦЕНЗИРОВАНИЯ / SECOND ROUND OF PEER-REVIEW
Авторы существенно доработали рукопись. Остался ряд замечаний, требующих внимания.
Необходимо добавить 5–7 ключевых слов, которые не дублируют напрямую формулировки названия статьи.
В текущей формулировке ключевые положения во многом носят характер обобщённых деклараций и лишь частично опираются на представленный клинический случай.
Первый пункт фактически описывает исход конкретного наблюдения (полный регресс неврологического дефицита после реимплантации катетера), не формулируя более общего практического вывода. Целесообразно переформулировать его в прикладном ключе, подчеркнув, что наблюдение демонстрирует возможность обратимости миграции катетера при своевременном проведении ревизионного вмешательства.
Второй и третий пункты выходят за рамки данных одного клинического случая и в настоящем виде звучат как категорические утверждения о необходимости пожизненного наблюдения и строгого ограничения показаний к операции Торкильдсена. Рекомендуется смягчить формулировки, придав им вероятностный характер (например: «данное наблюдение подчёркивает целесообразность длительного динамического наблюдения…», «полученные данные поддерживают точку зрения о необходимости более взвешенного подхода к выбору операции Торкильдсена…»), либо сопроводить их явными ссылками на литературные источники, демонстрирующие, что подобные выводы основаны не только на единичном клиническом случае.
Аннотация должна быть оформлена в соответствии с требованиями журнала (п.5.2 и 5.3 Правил для авторов; пример статьи на сайте - https://www.sechenovmedj.com/jour/article/view/1378/680 )
Описание случая не соответствует структуре CARE: отсутствует чётко выделенное введение (Background) в конце которого формулируется цель описания случая
В предложении «При катамнестическом обследовании через 10 лет…» необходимо указать, проводились ли методы визуализации (МРТ/КТ), и кратко описать их результаты и снимки.
Заявление о «первом в Российской Федерации задокументированном случае» требует более строгого обоснования: либо добавить краткое описание поиска по отечественным базам (RUSMED, eLIBRARY и др.), либо смягчить формулировку до «одного из первых описанных случаев».
Обсуждение.

8-2 Trubetskaya st., Moscow, 119048
Federal State Autonomous Educational Institution of Нigher Education I.M.Sechenov First Moscow State Medical University of the Ministry of Health of the Russian Federation (Sechenovskiy University)
E-mail: sechenovmedj@staff.sechenov.ru
Processing of personal data
































