




Contents
Scroll to:
https://doi.org/10.47093/2218-7332.2025.16.4.31-40
Scroll to:
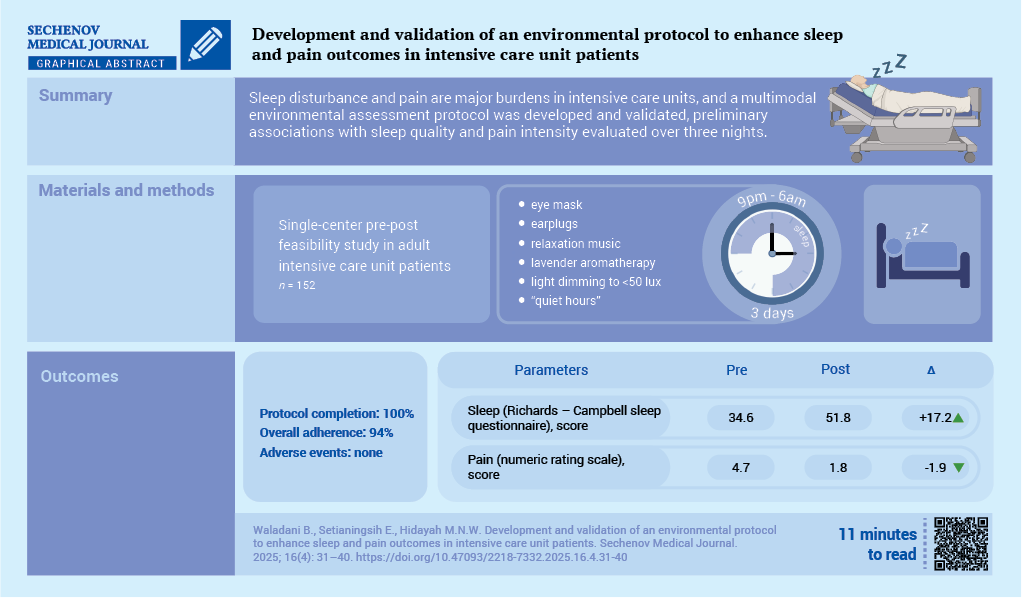
Aim. To develop a multimodal environmental modification protocol for the intensive care unit (ICU) and evaluate its feasibility and preliminary associations with sleep quality and pain intensity in patients.
Materials and methods. A quasi-experimental, single-arm study involving 152 adult patients was conducted from June to August 2025 in the ICU of a Type B hospital in Central Java, Indonesia. Environmental modifications included six interventions: earplugs, eye masks, music therapy, lavender aromatherapy, lighting adjustments, and noise reduction measures, which were applied daily for three consecutive nights (content validity = 0.94). Sleep quality was measured using the Richards-Campbell Sleep Questionnaire (RCSQ), and pain intensity was measured using the numeric rating scale (NRS). Paired t-tests, 95% confidence intervals (CI), and Cohen's d were used to describe intervention effectiveness. Normality of distribution was tested using the Shapiro–Wilk test.
Results. All 152 ICU participants completed the three-day protocol, with overall adherence being 94%. Mean RCSQ scores improved from 34.6 with 11.3 to 51.8 with 10.6 (95% CI: 15.46–18.94; paired t-test, p < 0.001; Cohen's d = 1.57). Mean NRS scores decreased from 4.7 with 1.8 to 2.8 with 1.3 (95% CI: −2.15 to −1.65; paired t-test, p < 0.001; Cohen's d = 1.21). No adverse events were noted. Objective environmental monitoring (subsample n = 40) showed a mean reduction in noise and lighting levels at the patient's bedside during the intervention.
Conclusion. The protocol for creating a positive environment in the ICU was feasible, acceptable, and resulted in subjective improvements in sleep quality and pain intensity in patients.
Abbreviations:
Sleep disturbance and pain management remain major issues in intensive care unit (ICU) worldwide [1][2]. A systematic review and meta-analysis A. Ashghab et al. [3] reported that approximately 66% of critically ill adult patients experienced sleep disturbance during their ICU stay, with these disturbances persisting for months after discharge. Another large observational study L. Alegria et al. [4] involving non-sedated ICU patients suggested that not only pain, but also environmental lighting, noise, and frequent nighttime care interventions were strongly correlated with poor sleep quality; similar findings have been reported previously [5][6]. Sleep disturbances have been linked to impaired respiratory performance, an increased risk of delirium, longer duration of mechanical ventilation, and higher ICU mortality [7–10].
Despite growing awareness, most interventions assessed in recent years focused on single-component strategies such as earplugs, eye masks, noise suppression, or music therapy [11][12]. In many studies, these interventions produced modest improvements, but standardization of combined environmental modification was lacking. Reviews called for multicomponent protocols, validated tools, and feasibility data to implementation guide [13]. Studies assessing the content validity of such interventions, adherence, and acceptability among ICU patients under real-world constraints were often lacking in healthcare settings in low- and middle-income countries [14–17].
The novelty of this study remained in designing integrated, validated environmental protocols and evaluating them for feasibility before large-scale trials. The development of intervention was informed by environmental theory in nursing, particularly the work of Florence Nightingale, which emphasizes the role of external factors such as light, noise, and ventilation in supporting patient recovery [18][19]. Concepts from behavioral sleep medicine, including stimulus control and relaxation theory, also guided the selection of intervention components [20–22]. By integrating these theoretical foundations, the protocol combined environmental modifications and sensory stimulation to create conditions conducive to improved sleep and reduced pain, thereby addressing the multifactorial challenges faced by ICU patients.
Aim of the study: to develop and clinically test a comprehensive environmental modification protocol in ICU and to evaluate its feasibility, acceptability, and preliminary associations with subjective sleep quality and pain intensity in adult patients. Secondary aims were to estimate effect sizes and to document adherence, safety, and operational issues relevant to the design of future randomized trials.
This study used a quasi-experimental, single-arm design with pre- and post-intervention feasibility assessment conducted between June and September 2025 in the ICU of a Type B accredited hospital in Central Java, Indonesia. Eligible patients were identified daily and consecutively recruited during the study period.
A total of 180 patients were screened between June and August 2025, of whom 152 met the inclusion criteria and were consecutively enrolled in the study (Fig.). 28 patients were excluded (did not meet criteria or declined).

FIG. TREND flowchart.
Note: ICU – intensive care unit; NRS – numeric rating scale; RCSQ – Richards-Campbell sleep questionnaire.
Inclusion criteria were:
Exclusion criteria were:
Lavender/essential oil allergy screening involved a baseline question regarding known allergies to fragrances or essential oils – patients with known allergy were excluded from the study. For patients without a known allergy a 5-minute bedside inhalation tolerance test was performed prior to the first night; if any adverse reactions occurred, aromatherapy was withheld.
The intervention protocol consisted of multiple non-pharmacological tools applied simultaneously: 1) Eye masks: soft cotton fabric eye masks (Lanaform, Belgium) with elastic bands, designed to block ambient light; 2) Earplugs: disposable polyurethane foam earplugs (3M™ 1100, USA) providing noise reduction rating of 29 dB; 3) Music therapy: instrumental relaxation music (tempo 60–80 beats per minute, volume 40–50 dB), delivered via bedside loudspeakers (Sony SRS-XB12, Japan). Music tracks were selected from a standardized relaxation playlist validated in prior ICU studies, consisting of slow-tempo instrumental music designed to promote relaxation and reduce environmental stress [23]; 4) Lavender aromatherapy: pure lavender essential oil (Lavandula angustifolia, Now Foods®, USA) diluted to 2% concentration in distilled water, was administered using an ultrasonic diffuser (InnoGear®, China) placed 1.5 m from the patient’s bed; 5) Lighting adjustment: overhead ICU fluorescent lamps were dimmed to <50 lux at patient bedside using adjustable dimmer switches installed in each cubicle; 6) Noise reduction: non-essential alarms and conversations near the patient were minimized. Staff were instructed to maintain voice levels <50 dB during nighttime hours. Noise reduction was implemented through staff education and the creation of an appropriate environment. ICU nurses received brief instructions to silence non-essential alarms when clinically appropriate, promptly responding to active alarms, and limiting non-urgent conversations at the patient's bedside during nighttime hours. Visual reminders were posted at the patient's bedside, and compliance with these rules was monitored by the nurse on duty during each shift.
The protocol was implemented over three consecutive nights from 21:00 to 06:00. Each night at 21:00, patients were assisted with the application of eye masks and earplugs, lavender aromatherapy diffuser was activated, lights were dimmed, and background music was played for 30 minutes prior to the sleep period. Earplugs and eye masks were maintained throughout the night unless removed by the patient. ICU staff adhered to a “quiet hours” policy to reduce avoidable disturbances. Intervention fidelity was monitored by bedside nurses and recorded in feasibility logs. The intervention was delivered individually at the bedside for each patient. All procedures were implemented by trained ICU nurses, under the supervision of the research team. To enhance protocol compliance, nurses assisted patients in applying earplugs and eye masks, monitored patient comfort throughout the night, and documented compliance using structured checklists. The individual ICU patient served as the unit of analysis, consistent with the unit of assignment.
Critical alarms remained active at all times. The protocol required that only non-critical alarms could be minimized (e.g., lowering non-urgent monitor volumes or relocating equipment alarms) while continuous physiological monitoring and rapid alarm escalation procedures were maintained. Nurses were instructed to immediately return devices to full volume if any clinical deterioration was observed. Adverse events (AE) were recorded using a structured AE log; trial staff reviewed logs daily. For aromatherapy intervention, patients underwent the pre-exposure tolerance check (5 minutes) under observation; any signs of respiratory distress, rash, or intolerance led to immediate discontinuation and reporting. No intervention-related AE occurred in this cohort.
The protocol, assessed by five experts, demonstrated high content validity across four criteria: relevance (1.00), clarity (0.92), simplicity (0.88), and applicability (0.96) with an overall average scale-level content validity index (S-CVI/Ave) of 0.94.
Data were collected using validated instruments to assess the feasibility of the intervention and its preliminary associations with sleep quality and pain intensity. Sleep quality was measured using the Richards-Campbell sleep questionnaire (RCSQ) [24], a widely used five-item visual analog scale ranging from 0 (very poor) to 100 (excellent): sleep depth, sleep latency, number of awakenings, efficiency of returning to sleep, and overall sleep quality. Pain intensity was evaluated daily using the numeric rating scale (NRS) [25], a simple and reliable tool in which patients rated their pain from 0 (no pain) to 10 (worst possible pain).
Primary feasibility outcomes were: recruitment rate, protocol completion (defined as participant completion of all 3 nights), per-component adherence (checklist), acceptability, and AE. Secondary exploratory outcomes: subjective sleep quality (RCSQ) and pain intensity (NRS). Objective environmental measures (bedside LAeq noise and bedside light level) were recorded in a subsample (n = 40) using calibrated instruments. The sample size was pragmatic for a feasibility study and included all eligible patients during the 3-month period (n = 152). No formal power calculation for hypothesis testing was performed; effect size estimates from this cohort will inform sample size calculations for future randomized controlled trials.
Blinding was not implemented in this study due to the nature of the intervention, which required ICU patients and nurses to be aware of the environmental modifications. Participants were informed of the interventions they received, and ICU nurses were responsible for administering and monitoring the protocol. Outcome assessment relied on validated self-report instruments (RCSQ and NRS), which minimized observer bias, but neither patients nor assessors were blinded to study condition.
Pre-post differences were assessed with paired t-tests (unless otherwise stated). Normality of difference scores was checked using Shapiro–Wilk tests; approximate normality supported use of parametric tests. We report means with standard deviations (SD), mean differences with 95% confidence intervals, paired t-statistics and p-values, and conservative Cohen’s d effect sizes calculated using the pooled SD: d = (Mean_post − Mean_pre) / SD_pooled, where SD_pooled = √[ (SD_pre² + SD_post²)/2]. For categorical pre-post changes (e.g., RCSQ category shifts), McNemar tests were used to formally assess whether observed category transitions were statistically significant beyond descriptive visualization. Missing data: none (all 152 completed). A significance level of α = 0.05 (two-tailed) was used. Data were analyzed using IBM SPSS Statistics 31.
A total of 152 adult patients were consecutively enrolled during the study period. Baseline characteristics are shown in Table 1. All 152 participants completed the full 3-night protocol (100% completion). Adherence was calculated as the proportion of scheduled components correctly delivered per patient across 3 nights (component checklist). Overall adherence was 94%. Component adherence (n = 152) included: eye mask 98%, earplug 96%, music therapy 92%, aromatherapy 94%, lighting adjustment 95%, staff quiet hours 88%. No intervention-related AE were recorded. Objective environmental monitoring in a subsample (n = 40) indicated reductions in bedside noise and light levels during intervention hours; however, quantitative logs were incomplete, so the results are presented descriptively.
Table 1. Demographic and clinical characteristics of intensive care unit patients
Variable | Value | % |
Age, years, mean ± SD | 56.2 ± 14.7 | |
Sex | ||
male, n (%) | 89 | 58.6 |
female, n (%) | 63 | 41.4 |
Diagnosis at admissiona | ||
stroke | 41 | 27.0 |
sepsis | 33 | 21.7 |
cardiac disease | 28 | 18.4 |
respiratory failure | 25 | 16.4 |
others | 25 | 16.4 |
Intensive care unit length of stay, days, mean ± SD | 6.8 ± 2.5 |
Notes: a presented as mutually exclusive primary diagnoses assigned at intensive care unit admission. Percentages do not represent a single diagnostic category because the study population consisted of patients with diverse clinical conditions admitted to the intensive care unit.
SD – standard deviation.
Sleep quality, measured by the RCSQ, increased markedly after the intervention, while pain intensity, assessed with the NRS, decreased substantially (Table 2). Both outcomes demonstrated large effect size estimates, indicating potential benefit within this feasibility context. Confidence intervals for mean changes indicated the precision of these estimates. No null or negative results were observed, and no mediation or causal inference analyses were performed, as the study was designed to assess feasibility and preliminary effects only.
Table 2. Changes in sleep quality and pain intensity before and after intervention
Outcome | Pre-intervention (Mean ± SD) | Post-intervention (Mean ± SD) | Mean difference | 95% CI | p-value | Cohen’s d |
RCSQ (sleep quality) | 34.6 ± 11.3 | 51.8 ± 10.6 | +17.2 | 15.46–18.94 | <0.001 | 1.57 |
NRS (pain intensity) | 4.7 ± 1.8 | 2.8 ± 1.3 | –1.9 | –2.15…–1.65 | <0.001 | 1.21 |
Note: CI – confidence intervals; NRS – numeric rating scale; RCSQ – Richards-Campbell sleep questionnaire; SD – standard deviation.
The clinical significance of these improvements is further illustrated in Table 3, which shows categorical shifts in outcome distributions. The proportion of patients reporting high sleep quality more than tripled, while the number experiencing mild pain nearly doubled. At the same time, the incidence of severe pain decreased significantly, demonstrating its clinical relevance within this feasibility context.
Table 3. Categorical changes in sleep quality and pain intensity pre- and post-intervention
Outcome (category) | Pre-intervention, n (%) | Post-intervention, n (%) | p-value |
RCSQ (Sleep quality) | |||
low (0–25) | 46 (30.3) | 17 (11.2) | <0.001 |
moderate (26–50) | 81 (53.3) | 56 (36.8) | |
high (>50) | 25 (16.4) | 79 (52.0) | |
NRS (Pain intensity) | |||
severe (7–10) | 29 (19.1) | 6 (3.9) | <0.001 |
moderate (4–6) | 86 (56.6) | 45 (29.6) | |
mild (1–3) | 37 (24.3) | 101 (66.5) |
Notes: p-values derived from McNemar tests assessing within-subject pre-post category changes.
NRS – numeric rating scale; RCSQ – Richards-Campbell sleep questionnaire.
This single-center feasibility study demonstrates that a standardized multimodal environmental protocol can be implemented with high completion and adherence rates in an ICU setting and is associated with preliminary, clinically meaningful improvements in patient-reported sleep quality and reductions in pain intensity. Given the single-arm design, these results should be interpreted as preliminary associations rather than as evidence of effectiveness. These results are consistent with our initial expectation that the protocol would be feasible, acceptable, and associated with preliminary improvements in patient outcomes. The absence of AE and the 100% completion rate suggest that the intervention was well tolerated, indicating that the protocol may be suitable for integration into routine ICU care pending further evidence [23–25]. Importantly, the large effect sizes observed highlight the potential value of environmental interventions when structured into a combined protocol.
The novelty of this study lies in the systematic development and validation of a protocol that integrated earplugs, eye masks, music therapy, aromatherapy, noise reduction, and lighting adjustment into a single intervention. Previous research has generally examined individual non-pharmacological components in isolation, such as earplugs, eye masks, music, or noise reduction strategies, often reporting modest or inconsistent effects on sleep and pain-related outcomes [26–28]. While fragmented interventions address only single aspects of the ICU environment, this multimodal approach integrates multiple strategies. In this feasibility study, the combined protocol was associated with larger pre- and post-intervention changes, although synergistic effects cannot be confirmed within the context of a single-arm feasibility design [29–31].
The observed improvements could be related to reductions in environmental stressors such as noise and light, as well as sensory and relaxation effects of aromatherapy and music therapy. However, alternative explanations cannot be ruled out, including reassurance and increased staff engagement [26][27]. These mechanisms align with previous international studies reporting improved sleep quality with earplugs and eye masks [11][12] and reduced anxiety and pain with music therapy and lavender inhalation [27][28][32]. However, increased patient calming and staff attention may also have contributed.
Implementation fidelity was high: adherence exceeded 94% and no safety concerns reported. Minor barriers included occasional discomfort from earplugs or masks, which required reassurance from nurses. Overall, these results underscore the feasibility of integrating environmental modifications into ICU workflows as a non-invasive, low-cost adjunct to pharmacological management. Clinically, such interventions have the potential to influence broader patient outcomes, as suggested by previous literature [33][34], although these aspects were not assessed in this feasibility study.
The intervention protocol demonstrated high feasibility and acceptability in this setting, suggesting its potential applicability to broader ICU environments pending further evaluation. Because the protocol consisted of simple, low-cost, and non-invasive environmental modifications, it could be readily adopted in a variety of healthcare settings, including hospitals in low- and middle-income countries where pharmacological options may be limited or carry greater risks. The high completion rate achieved without financial incentives underscores the relevance of these findings to real-world practice. Although the study was conducted in Type B hospital with a short follow-up period, the intervention components are universally applicable and can be easily integrated into ICU care packages worldwide. Future multicenter studies will be valuable to confirm these results and to guide global policy development in this area.
Key limitations include the single-center, single-arm pre-post study design, short follow-up period (three nights), subjective outcome measures, and potential expectancy/observer bias as the intervention was administered by staff and patients were informed about it. Objective measures were included for a subsample but full objective sleep assessment (actigraphy/polysomnography) and multicenter randomized controlled trials are recommended.
Future studies should employ randomized controlled designs with appropriate control groups to strengthen causal inference regarding the intervention’s potential effectiveness. To complement self-reported outcomes, objective measurements, such as actigraphy, polysomnography, or physiological biomarkers should be included. Multicenter trials are recommended to enhance generalizability of results across diverse ICU environments and patient populations. In addition, longer-term follow-up periods are needed to evaluate the sustained impact of environmental modifications on clinical recovery, delirium incidence, ICU length of stay, and post-discharge quality of life. Exploring cost-effectiveness and integration into standard ICU protocols may also provide valuable insights for broader implementation.
The validated multimodal environmental modification protocol demonstrated both feasibility and acceptability in this ICU study and was associated with significant improvements in patient-reported sleep quality (by 17.2% in 3 nights) and reductions in pain intensity (by 1.9% in 3 nights). These preliminary results support progression to larger randomized controlled trials with objective sleep measures and longer follow-up periods to evaluate potential effectiveness and generalizability.
Barkah Waladani was responsible for the study concept and design, conducted the experiment, and drafted the manuscript. Endah Setianingsih contributed to data acquisition, supported the implementation of the intervention, and participated in the critical revision of the manuscript. Muhammad N.W. Hidayah performed the statistical analysis, assisted in the analysis and interpretation of data, and contributed to the revision of the final manuscript. All authors approved the final version of the article.
Ethics statements. The study was conducted in accordance with the ethical principles outlined in the World Medical Association Declaration of Helsinki for biomedical research involving human subjects. The protocol was reviewed and approved by the Health Research Ethics Committee of Universitas Muhammadiyah Gombong, Approval No. 110.6/II.3. AU/F/KEPK/V/2025. Written informed consent was obtained from all patients included in the study or their legally authorized representatives.
Data availability. The data that support the findings of this study are available from the corresponding authors on reasonable request. Data and statistical methods used in the article were examined by a professional biostatistician on the Sechenov Medical Journal editorial staff.
Conflict of interest. The authors declare that there is no conflict of interests.
Financing. The study was supported by a research grant from the Ministry of Education, Culture, Research, and Technology of the Republic of Indonesia (Kemendiktisaintek), Grant No. 0070/C3/AL.04/20251.
1. List of Research Program Funding Recipients 2025, Indonesia. Number: 0070/C3/AL.04/2025. Grant No. 127/C3/DT.04.00/PL/2025 (access date: 12.12.2025).
1. Bolin M.C., Sweetman M.M. Sleep in the intensive care unit (ICU): an overlooked opportunity for occupational therapists to fill a gap in health care service. Open J Occup Ther. 2022; 10(1): 1–5. https://doi.org/10.15453/2168-6408.1846
2. Hillman D.R. Sleep loss in the hospitalized patient and its influence on recovery from illness and operation. Anesth Analg. 2021 May; 132(5): 1314–1320. https://doi.org/10.1213/ANE.0000000000005323. PMID: 33857973
3. Ashghab A., Vahedian-Azimi A., Vafadar Z., et al. Nursing interventions to improve the sleep quality of hospitalized patients: a systematic review and meta-analysis. Intensive Care Res. 2024; 4: 55–71. https://doi.org/10.1007/s44231-024-00056-9
4. Alegria L., Brockmann P., Repetto P., et al. Improve sleep in critically ill patients: study protocol for a randomized controlled trial for a multi-component intervention of environment control in the ICU. PLoS One. 2023 May; 18(5): e0286180. https://doi.org/10.1371/journal.pone.0286180. PMID: 37228142
5. Honarmand K., Bosma K.J. Risk factors for disrupted sleep in the ICU. In: Weinhouse G.L., Devlin J.W., editors. Sleep in Critical Illness. Cham: Springer; 2022. P. 91–108. https://doi.org/10.1007/978-3-031-06447-0_6
6. Vaishnav P.P., Suresh A., Kooragayalu S., Kooragayalu S. Sleep disturbances in hospitalized and intensive care unit patients. In: BaHammam A.S., Hunasikatti M., editors. Sleep Apnea Frontiers. Progress in Sleep Research. Singapore: Springer; 2023. P. 231– 253. https://doi.org/10.1007/978-981-99-7901-1_15
7. Li H.C., Yeh T.Y., Wei Y.C., et al. Association of incident delirium with short-term mortality in adults with critical illness receiving mechanical ventilation. JAMA Netw Open. 2022 Oct; 5(10): e2235339. https://doi.org/10.1001/jamanetworkopen.2022.35339. PMID: 36205994
8. Stollings J.L., Kotfis K., Chanques G., et al. Delirium in critical illness: clinical manifestations, outcomes, and management. Intensive Care Med. 2021 Oct; 47(10): 1089–1103. https://doi.org/10.1007/s00134-021-06503-1. Epub 2021 Aug 16. PMID: 34401939
9. Mart M.F., Williams Roberson S., Salas B., et al. Prevention and management of delirium in the intensive care unit. Semin Respir Crit Care Med. 2021 Feb; 42(1): 112–126. https://doi.org/10.1055/s-0040-1710572. Epub 2020 Aug 3. PMID: 32746469
10. Wu N., Zhang B., Wang Y., et al. Incidence, prevalence and risk factors of delirium in ICU patients: A systematic review and meta-analysis. Nurs Crit Care. 2023; 28: 653–669. https://doi.org/10.1111/nicc.12857
11. Waladani B., Utami W., Ernawati, Suwaryo P.A.W. Improving sleep quality among ICCU patients – evaluating the effectiveness of ear plug and eye mask interventions. Eur J Clin Exp Med. 2024; 22(4): 748–755. https://doi.org/10.15584/ejcem.2024.4.9
12. Bahcecioglu Turan G., Gürcan F., Özer Z. The effects of eye masks and earplugs on sleep quality, anxiety, fear, and vital signs in patients in an intensive care unit: a randomised controlled study. J Sleep Res. 2024 Apr; 33(2): e14044. https://doi.org/10.1111/jsr.14044. Epub 2023 Sep 18. PMID: 37723617
13. Holm A., Nikolajsen L., Dreyer P. A multicomponent intervention to optimise nurse–patient communication in the intensive care unit: a mixed-methods acceptability and feasibility study. Aust Crit Care. 2022 Nov; 35(6): 616–622. https://doi.org/10.1016/j.aucc.2021.09.008. Epub 2021 Nov 18. PMID: 34802842
14. Ijaz N., Nader M., Ponticiello M., et al. Contextual factors influencing bubble continuous positive airway pressure implementation for paediatric respiratory distress in low-income and middle-income countries: a realist review. Lancet Glob Health. 2025 Feb; 13(2): e232–e245. https://doi.org/10.1016/S2214-109X(24)00453-4. Epub 2024 Dec 12. PMID: 39675373
15. Rendon A., Luhning S., Bardin P., et al. Recommendations for improving discharge-related care following a COPD exacerbation: an expert panel consensus with emphasis on low- and middleincome countries. Int J Chron Obstruct Pulmon Dis. 2025 Apr; 20: 1111–1129. https://doi.org/10.2147/COPD.S502971. PMID: 40260081
16. Bartlett E.S., Lim A., Kivlehan S., et al. Critical care delivery across health care systems in low-income and low-middle-income country settings: a systematic review. J Glob Health. 2023 Dec; 13: 04141. https://doi.org/10.7189/jogh.13.04141. PMID: 38033248
17. Macey A., O'Reilly G., Williams G., Cameron P. Critical care nursing role in low and lower middle-income settings: a scoping review. BMJ Open 2022 Jan; 12(1): e055585. https://doi.org/10.1136/bmjopen-2021-055585. PMID: 34983772
18. Cardoso S.B., Oliveira I.C.S., Souza T.V., Carmo S.A. Pediatric intensive care unit: reflection in the light of Florence Nightingale’s environmental theory. Rev Bras Enferm. 2021; 74(5): e20201267. https://doi.org/10.1590/0034-7167-2020-1267. PMID: 34320154
19. Riegel F., Crossetti M.G.O., Martini J.G., Nes A.A.G. Florence Nightingale's theory and her contributions to holistic critical thinking in nursing. Rev Bras Enferm. 2021; 74(2): e20200139. https://doi.org/10.1590/0034-7167-2020-0139. PMID: 33950115
20. Shkodina A.D., Boiko D.I. A conception of integrated phased model combining sleep hygiene and stimulus control as an adult sleep education approach. Front Neurol. 2024 Dec; 15: 1513509. https://doi.org/10.3389/fneur.2024.1513509. PMID: 39744111
21. Edinger J.D., Arnedt J.T., Bertisch S.M., et al. Behavioral and psychological treatments for chronic insomnia disorder in adults: an American Academy of Sleep Medicine clinical practice guideline. J Clin Sleep Med. 2021 Feb; 17(2): 255–262. https://doi.org/10.5664/jcsm.8986. PMID: 33164742
22. Blampied N.M., van Deurs J. A conceptual framework for understanding and designing behavioral interventions for sleep problems in children on the autism spectrum. In: McLay L.K., France K.G., Blampied, N.M., editors. Clinical Handbook of Behavioral Sleep Treatment in Children on the Autism Spectrum. Cham: Springer; 2022. P. 59–74. https://doi.org/10.1007/978-3-030-99134-0_5
23. Kakar E., Ottens T., Stads S., et al. Effect of a music intervention on anxiety in adult critically ill patients: a multicenter randomized clinical trial. J Intensive Care. 2023 Aug; 11(1): 36. https://doi.org/10.1186/s40560-023-00684-1. PMID: 37592358
24. Richards K.C., O’Sullivan P.S., Phillips R.L. Measurement of sleep in critically ill patients. J Nurs Meas. 2000 Fall-Winter; 8(2): 131–144. PMID: 11227580
25. Breivik H., Borchgrevink P.C., Allen S.M., et al. Assessment of pain. Br J Anaesth. 2008 Jul; 101(1): 17–24. https://doi.org/10.1093/bja/aen103. Epub 2008 May 16. PMID: 18487245
26. Wu T., Qi H., Hui K., et al. Effect of noise isolation with noisecancelling earmuffs during laparoscopic surgery on acute postoperative pain: a clinical randomised controlled trial. BMC Anesthesiol. 2025 Oct; 25(1): 498. https://doi.org/10.1186/s12871-025-03369-4. PMID: 41087929
27. Hu L., Wang E.J. Sleep as a therapeutic target for pain management. Curr Pain Headache Rep. 2023 Jun; 27(6): 131–141. https://doi.org/10.1007/s11916-023-01115-4. Epub 2023 May 10. PMID: 37162641
28. Rampes S., Ma K., Divecha Y.A., et al. Postoperative sleep disorders and their potential impacts on surgical outcomes. J Biomed Res. 2019 Aug; 34(4): 271–280. https://doi.org/10.7555/JBR.33.20190054. PMID: 32519977
29. Bienefeld N., Keller E., Grote G. AI interventions to alleviate healthcare shortages and enhance work conditions in critical care: qualitative analysis. J Med Internet Res. 2025 Jan; 27: e50852. https://doi.org/10.2196/50852. PMID: 39805110
30. McNelly A., Langan A., Bear D.E., et al. A pilot study of alternative substrates in the critically Ill subject using a ketogenic feed. Nat Commun. 2023 Dec; 14(1): 8345. https://doi.org/10.1038/s41467-023-42659-8. PMID: 38102152
31. Zhang X.L., Zhang X., Hua W., et al. Expert consensus on the diagnosis, treatment, and prevention of respiratory syncytial virus infections in children. World J Pediatr. 2024 Jan; 20(1): 11–25. https://doi.org/10.1007/s12519-023-00777-9. Epub 2023 Dec 8. Erratum in: World J Pediatr. 2024 Feb 25. https://doi.org/10.1007/s12519-023-00792-w. PMID: 38064012
32. Whale K., Dennis J., Wylde V., et al. The effectiveness of nonpharmacological sleep interventions for people with chronic pain: a systematic review and meta-analysis. BMC Musculoskelet Disord. 2022 May; 23(1): 440. https://doi.org/10.1186/s12891-022-05318-5. PMID: 35546397
33. Chlan L.L., Weinert C.R., Heiderscheit A., et al. Effects of Patient-Directed Music Intervention on Anxiety and Sedative Exposure in Critically Ill Patients Receiving Mechanical Ventilatory Support: A Randomized Clinical Trial. JAMA. 2013 Jun; 309(22): 2335– 2344. https://doi.org/10.1001/jama.2013.5670. PMID: 23689789
34. Devlin J.W., Skrobik Y., Gélinas C., et al. Clinical Practice Guidelines for the Prevention and Management of Pain, Agitation/ Sedation, Delirium, Immobility, and Sleep Disruption in Adult Patients in the ICU. Crit Care Med. 2018 Sep; 46(9): e825–e873. https://doi.org/10.1097/CCM.0000000000003299. PMID: 30113379
Barkah Waladani, Assistant Professor, Department of Critical Care Nursing, Faculty of Health and Science
461, Yos Sudarso str., Gombong, Kebumen, 54412
Endah Setianingsih, Senior Lecturer, Department of Critical Care Nursing, Faculty of Health and Science
461, Yos Sudarso str., Gombong, Kebumen, 54412
Muhammad N.W. Hidayah, Senior Lecturer, Department of Industrial Engineering, Faculty of Science and Humanities
461, Yos Sudarso str., Gombong, Kebumen, 54412
Sechenov Medical Journal. Editor's checklist for this article you can find here.
Журнал «Сеченовский вестник» |
| Sechenov Medical Journal |
Рецензии на рукопись |
| Peer-review reports |
Название / Title | Разработка и валидация протокола модификации окружающей среды, влияющей на качество сна и интенсивность боли у пациентов отделения интенсивной терапии / Development and validation of an environmental protocol to enhance sleep and pain outcomes in intensive care unit patients
|
Раздел / Section
| ХИРУРГИЯ/ SURGERY
|
Тип / Article | Оригинальная статья / Original article |
Номер / Number | 1354
|
Страна/территория / Country/Territory of origin | Индонезия / Indonesia |
Язык / Language | Английский / English
|
Источник / Manuscript source | Инициативная рукопись / Unsolicited manuscript |
Дата поступления / Received | 03.10.2025
|
Тип рецензирования / Type ofpeer-review | Двойное слепое / Double blind |
Язык рецензирования / Peer-review language | Английский / English
|
РЕЦЕНЗЕНТ А / REVIEWER A
Инициалы / Initials | 1354_А
|
Научная степень / Scientific degree | Кандидат медицинских наук / PhD
|
Страна/территория / Country/Territory | Малайзия / Malaysia
|
Дата рецензирования / Date of peer-review | 05.12.2025 |
Число раундов рецензирования / Number of peer-review rounds | 2 |
Финальное решение / Final decision | Принять к публикации / accept
|
ПЕРВЫЙ РАУНД РЕЦЕНЗИРОВАНИЯ / FIRST ROUND OF PEER-REVIEW
Scientific quality: Grade C: Good
Language quality: Grade B: Minor language polishing
Overall assessment: The study addresses an important issue which is improving sleep and pain outcomes in ICU patients through environmental modification. However, several methodological, statistical, and reporting weaknesses limit the validity of the findings. Major revision is required before the paper can be considered for publication.
Major Comments
Study Design:
Sampling & Participants:
Safety & Ethics:
Statistical Issues:
Adherence & Feasibility:
Data Transparency:
Minor Comments
The study is feasible and relevant but must clarify methodology, correct statistical reporting, and ensure patient safety and transparency before publication.
CONCLUSION: major revision.
THE SECOND ROUND OF PEER REVIEW
All reviewer's comments have been addressed by the authors.
Recommended for publication.
РЕЦЕНЗЕНТ B / REVIEWER B
Инициалы / Initials | 1354_В
|
Научная степень / Scientific degree | Кандидат медицинских наук / PhD
|
Страна/территория / Country/Territory | Индонезия / Indonesia
|
Дата рецензирования / Date of peer-review | 03.12.2025 |
Число раундов рецензирования / Number of peer-review rounds | 2 |
Финальное решение / Final decision | Переработка и повторное рецензирование / major revision |
ПЕРВЫЙ РАУНД РЕЦЕНЗИРОВАНИЯ / FIRST ROUND OF PEER-REVIEW
Scientific quality: Grade C: Good
Language quality: Grade B: Minor language polishing
This study explores an important and under-researched area in critical care nursing — the use of multimodal environmental modification to enhance patient comfort, sleep, and pain control. The manuscript is well organized, clear, and supported by relevant literature. However, several substantive revisions are needed to strengthen scientific rigor and alignment with the study design.
Major points for revision:
In addition to this review text, please view the reviewer's comments in the attached file with the text of your manuscript.
CONCLUSION: major revision.
THE SECOND ROUND OF PEER REVIEW
Unfortunately, the reviewer did not respond to the editorial repeated requests.
РЕКОМЕНДАЦИИ НАУЧНЫХ РЕДАКТОРОВ ЖУРНАЛА / RECOMMENDATIONS
OF THE SCIENTIFIC EDITORS OF THE JOURNAL
Title
Spell out the ICU abbreviation in the title as “intensive care unit” instead of using only “ICU”.
Introduction
Shorten the Introduction, remove repetitive wording and self‑evident statements, and strengthen the focus on: the burden of sleep disturbances and pain in intensive care units, the lack of multicomponent protocols, especially in low‑ and middle‑income countries (LMICs).
Clearly formulate the aim of the study at the end of the Introduction.
Materials and methods
Standardize the description of the study design; rewrite the “Sampling”/“Recruitment” section to avoid wording suggestive of convenience sampling and to emphasize consecutive recruitment of all eligible patients during the study period.
Clearly separate inclusion criteria, exclusion criteria, and the screening algorithm.
Clarify the intervention protocol by:
Standardize the description of materials (brand/model of eye masks, earplugs, diffuser, music tracks) in line with journal style, avoiding unnecessary commercial details.
Describe content validation of the protocol more clearly (approach, indices, thresholds).
Distinguish primary and secondary outcomes explicitly.
Expand the statistical analysis section to:
Explain the rationale for the sample size in the context of a feasibility study.
Results
Restructure the Results section into logical subsections (e.g. baseline characteristics, feasibility outcomes, clinical outcomes, categorical changes), ensuring a clear sequence and alignment with tables and figures.
Discussion, limitations, future directions
Reduce the strength of claims about “synergistic effects” and “strong impact”, replacing them with more cautious wording such as “potential benefit” and “large pre‑post changes within a feasibility context”.
Separate the “Limitations” and “Directions for further research” sections, with a clear list of methodological limitations (single‑center, single‑arm design, short follow‑up, subjective outcomes, lack of blinding).
Tables, figures, language
Bring all tables and figures into a unified journal style:
Carefully revise the text for syntax and terminology (ICU, feasibility, adherence, environmental modification), avoiding repetition and overly complex sentences.

8-2 Trubetskaya st., Moscow, 119048
Federal State Autonomous Educational Institution of Нigher Education I.M.Sechenov First Moscow State Medical University of the Ministry of Health of the Russian Federation (Sechenovskiy University)
E-mail: sechenovmedj@staff.sechenov.ru
Processing of personal data
































