




Contents
Scroll to:
https://doi.org/10.47093/2218-7332.2025.16.3.40-47
Scroll to:
Microsurgical treatment of ocular artery aneurysms is classified as high-risk surgery. It is anatomically impossible to prevent and stop bleeding from ophthalmic aneurysms by applying a standard clip proximal to the aneurysm.
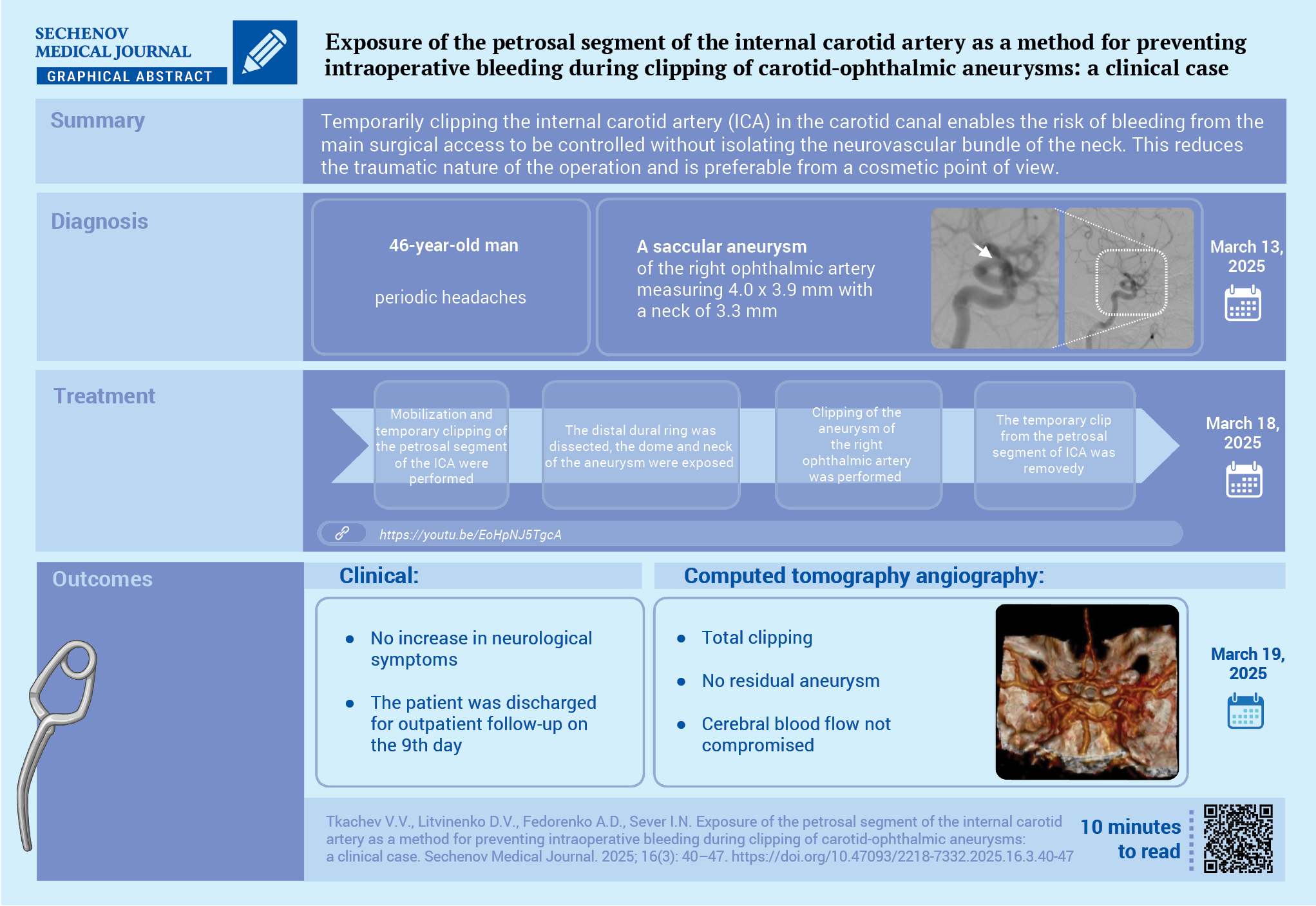
Case report. A 46-year-old man was admitted complaining of periodic headaches for 6 months. Outpatient magnetic resonance imaging revealed an aneurysm of the right internal carotid artery (ICA). According to computed tomography and cerebral angiography, an aneurysm of the ocular artery was verified. The patient chose an open surgery from the proposed treatment methods. Clipping of the aneurysm of the ocular artery mouth was performed by pterion access with an extradural extraction of the petrosal segment of the ICA to prevent intraoperative bleeding. The course of the postoperative period was smooth, without neurological symptoms, and the stitches were removed on the 9th day. The patient was discharged under outpatient supervision with a recommendation to control the radicality of clipping after 6 months.
Discussion. Temporary clipping of the ICA in the carotid canal during microsurgical operations for ocular artery aneurysms allows controlling the risk of bleeding from the main surgical access without isolating the neurovascular bundle of the neck, which reduces the traumatic nature of the operation and is preferable from a cosmetic point of view.
Abbreviations:
Open exclusion of carotid-ophthalmic aneurysms is a non-trivial task due to the peculiarities of their anatomy [1], inaccessibility, difficulty in stopping possible bleeding from the aneurysm, as well as the risks of deterioration of visual functions [2]. Currently, the choice of treatment for ophthalmic aneurysms is intravascular interventions, but a significant proportion of patients continue to undergo open surgeries for various reasons [3].
The issue of prevention and effective control of bleeding remains a cornerstone of microsurgery for ophthalmic aneurysms. Proximal bleeding control is traditionally achieved by dissecting the cervical segment of the internal carotid artery (ICA), which de facto means performing an additional operation with potential complications and cosmetic defects [4]. The use of temporary clipping of the ICA in the carotid canal allows for the effective cessation of antegrade blood flow in the proximal segments of the ICA without dissection of the cervical neurovascular bundle, thereby reducing the trauma of the operation and the risks of perioperative complications and improving cosmetic results [5–7].
The aim of this case report is to demonstrate the experience of temporary clipping of the ICA in the carotid canal using an open approach during microsurgical exclusion of an aneurysm of the right ophthalmic artery.
A 46-year-old patient was admitted to the clinic of the Scientific Research Institute – Regional Clinical Hospital No. 1 named after Prof. S. V. Ochapovsky on March 13, 2025. The patient complained of periodic headaches that had been bothering him for the past six months. An outpatient magnetic resonance imaging scan of the brain revealed an aneurysm of the right ICA. The patient was hospitalized for digital subtraction cerebral angiography and surgical treatment. On examination: the neurological status without focal neurological symptoms, the somatic status without abnormalities. Computed tomography angiography and cerebral angiography verified a saccular aneurysm of the right ophthalmic artery measuring 4.0×3.9 mm with a neck of 3.3 mm (Fig. 1A–D).

FIG. 1. Computed tomography (A), computed tomography angiography (B, C), and cerebral angiography (D) of a 46-year-old patient with an aneurysm of the ophthalmic artery orifice befo e surgery.
A, B. Axial section: aneurysm dome (arrow), no signs of hemorrhage.
C. 3D reconstruction: 1 – aneurysm dome, 2 – M2 segment of the middle cerebral artery, 3 – C7 segment of the internal carotid artery.
D. Lateral projection: aneurysm dome (arrow).
After consultation with endovascular surgeons, the patient was offered a choice: endovascular treatment using an intracranial stent or open aneurysm exclusion. The potential risks of open and endovascular treatment were explained. The patient preferred open surgery and signed the relevant consent form.
The operation was performed on March 18, 2025. A limited incision of the dura mater was made using the standard pterional approach. The cistern of the lateral cerebral fossa (Sylvian cistern) was opened to relax the brain. An extradural subfrontal approach was used to resect the lesser wing of the sphenoid bone and remove the anterior clinoid process. Hemostasis was achieved. After the final opening of the dura mater and dissection of the basal cisterns, the optic nerve, ICA, and aneurysm dome were identified.
An extradural subtemporal approach to the anterior surface of the temporal bone pyramid was performed to ensure proximal control of possible bleeding. The foramen spinosum and foramen ovale were identified. Partial peeling of the outer wall of the cavernous sinus was performed, exposing the mandibular nerve. The greater petrosal nerve was identified.
After skeletonization of the apex of the petrous bone and trepanation of the upper wall of the carotid canal (Fig. 2A), mobilization and temporary clipping of the petrosal segment of the ICA were performed (Fig. 2B). Then the distal dural ring was dissected, the dome and neck of the aneurysm were exposed (Fig. 2C). Clipping of the aneurysm of the right ophthalmic artery was performed (Fig. 2D). After checking the patency of the ophthalmic artery, coagulation of the aneurysm dome was performed. The temporary clip from the ICA was removed, hemostasis was achieved in the area of the petrous segment of the ICA, and the surgical wound was sutured. A video of the operation is available at the link: https://youtu.be/EoHpNJ5TgcA.

FIG. 2. Clipping of the aneurysm of the right ophthalmic artery orifice in a 46-year-old patient.
A. Removal of the superior wall of the carotid canal, exposure of the petrous segment of the internal carotid artery (arrow).
B. Temporary clipping of the C2 internal carotid artery (arrow).
C. Dissection of the aneurysm of the ophthalmic artery orifice: 1 – optic nerve, 2 – aneurysm dome, 3 – internal carotid artery.
D. Clipping of the ophthalmic artery aneurysm (arrow).
The postoperative period was uneventful, with no increase in neurological symptoms. Follow-up computed tomography and сomputed tomography angiography scans performed one day after surgery (March 19, 2025) revealed no residual aneurysm (Fig. 3A–C). The wound healed by primary tension, the sutures were removed on the 9th day, and the patient was discharged for outpatient follow-up with a recommendation to check the radicality of clipping in 6 months.

FIG. 3. Computed tomography (A), computed tomography angiography (B, C) of a 46-year-old patient with an aneurysm of the ophthalmic artery ostium 24 hours after surgery. Total clipping, cerebral blood flow not compromised.
A, B. Axial section: clip on the aneurysm (arrow).
C. 3D reconstruction: clip on the aneurysm (arrow).
Performing open surgeries on cerebral aneurysms is associated with an increased risk of intraoperative bleeding during dissection of the aneurysm dome and neck [8].
Patients with ophthalmic artery aneurysms, which are anatomically complex and difficult to access for surgery, are operated on mostly using intravascular methods. These include occlusion using microcoils: balloon and stent assistance, as well as the installation of flow-diverting devices [9–11].
In open surgery, prevention and control of bleeding from intradural and transit aneurysms of the ophthalmic segment of the ICA are particularly important, since routine application of temporary clips proximal to the aneurysm is impossible due to anatomical conditions. To date, the main method for controlling bleeding from ophthalmic aneurysms remains the exposure of the bifurcation of the common carotid artery into the internal and external branches in the neck. This method of proximal control involves the use of a second surgical approach with possible complications: paresis of the vocal cords and tongue; hematoma in the surgical area, causing compression of the trachea and severe breathing difficulties, in some cases requiring intubation or tracheostomy; dissection of the exposed arteries. Access to the neck vessels may be difficult or impossible in the presence of cicatricial adhesive process after previous surgery or radiation therapy [4].
Occlusion of the ICA in the neck often does not lead to complete cessation of antegrade blood flow through the ophthalmic segment, which is associated with the presence of distal anastomoses between the ICA and branches of other brachiocephalic arteries [12].
Methods for mobilizing the ICA proximal to its cerebral portion, in the ICA carotid canal, were proposed quite some time ago [6][7], but they did not become widely used due to the complexity of their technical implementation and the presence of a number of shortcomings. The intradural access to the petrosal part of the ICA proposed by T.M. Wascher et al. [6], involved complete mobilization of the temporal lobe pole, which significantly increased the risk of developing venous cerebral infarction in the surgical area, and the use of a balloon catheter for occlusion of the ICA carried the risks of incomplete occlusion or excessive compression, leading to damage to the arterial wall.
In the technique described by L.N. Sekhar et al. [7], orbitomaxillofacial craniotomy was proposed for the isolation of the petrosal segment of the ICA, which made the operation more traumatic and worsened cosmetic results. In addition, in all cases, when drilling the carotid canal in the posterolateral triangle (Glasscock triangle) required opening the bony part of the auditory tube, which increased the risk of developing inflammation of the middle ear inflammation and hearing loss. Both techniques involved transection of the greater petrosal nerve, creating a potential risk of complications due to denervation of the lacrimal gland on the access side.
In the described case, a modified method of proximal bleeding control was used (video) [5]. To perform this procedure, after standard pterional craniotomy, the upper wall of the carotid canal in the posteromedial triangle (Kawase triangle) is resected using an extradural approach. The roots of the trigeminal and greater petrosal nerves are preserved; the Eustachian tube, cochlea, and internal auditory canal remain intact. The ICA is mobilized in a sheath of periosteum lining the walls of the carotid canal, which minimizes its trauma, and occlusion of the ICA with clips with a specified degree of compression of their branches reliably stops blood flow without damaging the vascular wall.
The use of modern methods of proximal bleeding control during open surgery in patients with aneurysms of the ophthalmic segment of the ICA, including temporary clipping of the petrosal segment of the ICA, allows for the optimization of surgical technique. This results in increasing the safety of the intervention due to the reliable prevention of bleeding, as well as minimizing the amount of tissue trauma, and improving cosmetic and functional outcomes. All of these factors are important for the patient’s quality of life.
Vyacheslav V. Tkachev performed the surgery, made the main contribution to the concept and design of the article, and supervised the writing and editing process. Dmitry V. Litvinenko, Arkady D. Fedorenko participated in the development of the concept and design of the article, writing and editing the text, as well as preparing illustrations and video. Irina N. Sever participated in the analysis of literature data, processing of illustrations and video, editing the text. All authors approved the final version of the article.
Compliance with ethical standards. Consent statement. The patient consented to the publication of the article “Exposure of the petrous segment of the internal carotid artery as a method for prevention of intraoperative bleeding during clipping of carotid-ophthalmic aneurysms: a clinical case” in the “Sechenov Medical Journal”.
Conflict of interests. The authors declare that there is no conflict of interests.
Financing. The study was not sponsored (own resources).
1. Sever I.N., Gerasyuta A.E., Litvinenko D.V., Tkachev V.V. Classification of ophthalmic segment internal carotid artery aneurysms: a literature review. Sechenov Medical Journal. 2024; 15(4): 4–18 (In Russian). https://doi.org/10.47093/2218-7332.2024.15.4.4-18. EDN: IGGXRN
2. Rahmanian A., Mohammad Hosseini E., Sourani A., et al. Microsurgical treatment of ophthalmic artery aneurysm, a case series of 55 patients with long-term follow-up. BMC Surg. 2024 May; 24(1): 139. https://doi.org/10.1186/s12893-024-02419-x. PMID: 38714953
3. Luzzi S., Del Maestro M., Galzio R. Microneurosurgery for Paraclinoid Aneurysms in the Context of Flow Diverters. Acta Neurochir Suppl. 2021; 132: 47–53. https://doi.org/10.1007/978-3-030-63453-7_7. PMID: 33973028
4. Jani P., Mathuriya S.N., Dhandapani S. Safe Cervical ICA Control for Clipping Clinoid-Ophthalmic Segment ICA Aneurysms. Turk Neurosurg. 2021; 31(5): 821–822. https://doi.org/10.5137/1019-5149.JTN.32688-20.1. PMID: 34169987
5. Tkachev V.V., Litvinenko D.V., Sever I.N., et al. Patent of the Russian Federation RU 2 823 205 C1 Method for the Prevention and Control of Bleeding from Aneurysms of the Ophthalmic Segment of the Internal Carotid Artery. Published: 22.07.2024 Bul. No. 21.
6. Wascher T.M., Spetzler R.F., Zabramski J.M. Improved transdural exposure and temporary occlusion of the petrous internal carotid artery for cavernous sinus surgery. Technical note. J Neurosurg. 1993 May; 78(5): 834–837. https://doi.org/10.3171/jns.1993.78.5.0834. PMID: 8468617
7. Sekhar L.N., Sen C.N., Jho H.D. Saphenous vein graft bypass of the cavernous internal carotid artery. J Neurosurg. 1990 Jan; 72(1): 35–41. https://doi.org/10.3171/jns.1990.72.1.0035. PMID: 2294182
8. Tawk R.G., Hasan T.F., D’Souza C.E., et al. Diagnosis and Treatment of Unruptured Intracranial Aneurysms and Aneurysmal Subarachnoid Hemorrhage. Mayo Clin Proc. 2021 Jul; 96(7): 1970–2000. https://doi.org/10.1016/j.mayocp.2021.01.005. Epub 2021 May 13. PMID: 33992453
9. Silva M.A., See A.P., Dasenbrock H.H., et al. Vision outcomes in patients with paraclinoid aneurysms treated with clipping, coiling, or flow diversion: a systematic review and meta-analysis. Neurosurg Focus. 2017 Jun; 42(6): E15. https://doi.org/10.3171/2017.3.FOCUS1718. PMID: 2856598
10. Kanemaru K., Yoshioka H., Hashimoto K., et al. Treatment of Unruptured Large and Giant Paraclinoid Aneurysms in Japan at the Time of Flow Diverter Introduction: A Nationwide, Multicenter Survey by the Japanese Society on Surgery for Cerebral Stroke. World Neurosurg. 2025 Mar; 195: 123571. https://doi.org/10.1016/j.wneu.2024.123571. Epub 2025 Jan 17. PMID: 39681259
11. Behari S., Dikshit P., Singh S., et al. Paraclinoid Segment Aneurysms of the Internal Carotid Artery: Surgical Clipping. Neurol India. 2021 Sep-Oct; 69(5): 1184–1195. https://doi.org/10.4103/0028-3886.329547. PMID: 34747782
12. Babichev K.N., Savello A.V., Svistov D.V., et al. Segmental agenesis of the cervical internal carotid artery with collateral blood supply from the ascending pharyngeal artery and intercavernous anastomosis: a clinical case and literature review. Burdenko’s Journal of Neurosurgery. 2018; 82(2): 81–87. https://doi.org/10.17116/oftalma201882281-87. PMID: 29795090
Vyacheslav V. Tkachev, Dr. of Sci. (Medicine), Professor, Department of Neurology and Neurosurgery, Associate Professor, Department of Surgery No. 1, Kuban State Medical University; Head of the Department of Neurosurgery No. 2, SRI – Regional Clinical Hospital No. 1 named after prof. S.V. Ochapovsky
167, 1 May str., Krasnodar, 350086,
4, Mitrofan Sedin str., Krasnodar, 350063
Dmitry V. Litvinenko*, Cand. of Sci. (Medicine), neurosurgeon, Department of Neurosergery No. 2
167, 1 May str., Krasnodar, 350086
Arkady D. Fedorenko, resident, Department of Neurology and Neurosurgery
4, Mitrofan Sedin str., Krasnodar, 350063
Irina N. Sever, postgraduate student, Department of Neurology and Neurosurgery
4, Mitrofan Sedin str., Krasnodar, 350063
Sechenov Medical Journal. Editor's checklist for this article you can find here.
Журнал «Сеченовский вестник» |
| Sechenov Medical Journal |
Рецензии на рукопись |
| Peer-review reports |
Название / Title | Выделение петрозального сегмента внутренней сонной артерии как метод профилактики интраоперационного кровотечения при клипировании каротидно- офтальмических аневризм: клинический случай/ Exposure of the petrosal segment of the internal carotid artery as a method for preventing intraoperative bleeding during clipping of carotid-ophthalmic aneurysms: a clinical case |
Раздел / Section
| НЕЙРОХИРУРГИЯ/ NEUROSURGERY
|
Тип / Article | Клинический случай / Сlinical case |
Номер / Number | 1267
|
Страна/территория / Country/Territory of origin | Россия / Russia |
Язык / Language | Английский / English
|
Источник / Manuscript source | Инициативная рукопись / Unsolicited manuscript |
Дата поступления / Received | 04.06.2025 |
Тип рецензирования / Type ofpeer-review | Двойное слепое / Double blind |
Язык рецензирования / Peer-review language | Английский /Русский/ English /Russian |
РЕЦЕНЗЕНТ А / REVIEWER A
Инициалы / Initials | 1267_А
|
Научная степень / Scientific degree | Доктор медицинских наук / Dr. of Sci. (Medicine)
|
Страна/территория / Country/Territory | Россия / Russia
|
Дата рецензирования / Date of peer-review | 06.07.2025 |
Число раундов рецензирования / Number of peer-review rounds | 1 |
Финальное решение / Final decision | принять к публикации / accept
|
ПЕРВЫЙ РАУНД РЕЦЕНЗИРОВАНИЯ / FIRST ROUND OF PEER-REVIEW
Аневризмы офтальмического сегмента внутренней сонной артерии (ВСА) традиционно рассматриваются в качестве сложных, в связи с особенностями их анатомического строения, труднодоступностью для открытой хирургии и наличием риска ухудшения зрительных функций. Улучшение результатов хирургического лечения пациентов с церебральными аневризмами, которые относятся к категории сложных, остается актуальной проблемой нейрохирургии. Аневризмы, располагающиеся в офтальмическом сегменте внутренней сонной артерии, относят к сложным в связи с особенностями их анатомического строения и труднодоступностью для открытой хирургии.
Рукопись соответствует правилам этики проведения исследований и публикации их результатов. На современном этапе нейрохирургии лечение такой патологии требует комбинации различных методов лечения — применения базальных доступов, этапного ремоделирования широкой шейки ВСА, клипирования и эндоваскулярного лечения в условиях гибридной рентген-операционной. И это авторами показано подробно и поэтапно.
Использование научной терминологии и ее соответствие принятой в рассматриваемой области знаний соответствует современной терминологии данного раздела представленной работы: клипирования аневризмы устья глазной артерии птериональным доступом с экстрадуральным выделением петрозального сегмента ВСА с целью профилактики интраоперационного кровотечения. Это один из очень трудных и рискованных доступов, с которым авторы справились отлично.
Авторы акцентировали внимание на одной из ключевых характеристик сложных ВСА — их труднодоступности. Часть ВСА относят к сложным аневризмам из-за таких характеристик, как анатомия ВСА и тяжесть состояния больного.
Сложная ВСА не может быть вылечена одним каким-либо методом, например, клипированием ВСА с применением только стандартного нейрохирургического доступа или с использованием только эндоваскулярного лечения. Лечение сложных ВСА требует применения комбинированного лечения —клипирование ВСА с применением различных доступов. сочетание этапного ремоделирование.
ЗАКЛЮЧЕНИЕ: принять к публикации.
РЕЦЕНЗЕНТ B / REVIEWER B
Инициалы / Initials | 1267_В
|
Научная степень / Scientific degree | Кандидат медицинских наук / PhD |
Страна/территория / Country/Territory | Россия/ Russia
|
Дата рецензирования / Date of peer-review | 15.07.2025 |
Число раундов рецензирования / Number of peer-review rounds | 1 |
Финальное решение / Final decision | принять к публикации после небольшой доработки / minor revision
|
ПЕРВЫЙ РАУНД РЕЦЕНЗИРОВАНИЯ / FIRST ROUND OF PEER-REVIEW
Рукопись посвящена описанию хирургической технике редкой и труднодоступной локализации аневризм головного мозга (параклиноидной аневризме). Авторы представили клинический случай, сопровождающийся подробным описанием хирургического вмешательства, что делает работу актуальной и полезной для специалистов в области нейрохирургии, эндоваскулярной хирургии, неврологии и радиологии.
По сути, представлен хирургической доступ к петрозальному сегменту сонной артерии для временного клипирования и контроля кровотечения во время диссекции и наложения постоянной клипсы на параклиноидную аневризму внутренней сонной артерии (ВСА).
Данный метод подробно описан несколькими авторами интрадуральным и эктрадуральным доступом. Новых технологий не предлагается, но с технической стороны читателям будет интересен такой подход, так как классический доступ к эктракраниоальному отделу ВСА в области сонного треугольника и так называемый аспирационный метод не всегда позволяет контролировать кровотечение и связан с дополнительным доступом вне операционной раны – на шейном отделе.
Вместе с тем остаётся ряд вопросов и замечаний, требующих уточнения и доработки:
Для более наглядного представления и точной идентификации анатомических ориентиров целесообразно дополнить рукопись современными иллюстративными публикациями с элементами анатомической диссекции. Это позволит более чётко выделить и корректно подписать ключевые анатомические структуры, связанные с используемым хирургическим доступом.
В качестве примера современной и методически ценной работы может быть использована публикация:
Benet A., Salinas R., Bustos Andrade A., Mura J. Minimally Invasive Posterolateral Transcavernous Transtentorial Approach: 2-Dimensional Operative Video. Operative Neurosurgery. 2023;25(2):e78. DOI: 10.1227/ons.0000000000000671.
ЗАКЛЮЧЕНИЕ: принять к публикации после небольшой доработки.
РЕКОМЕНДАЦИИ НАУЧНЫХ РЕДАКТОРОВ ЖУРНАЛА / RECOMMENDATIONS
OF THE SCIENTIFIC EDITORS OF THE JOURNAL
Текст
Видео

8-2 Trubetskaya st., Moscow, 119048
Federal State Autonomous Educational Institution of Нigher Education I.M.Sechenov First Moscow State Medical University of the Ministry of Health of the Russian Federation (Sechenovskiy University)
E-mail: sechenovmedj@staff.sechenov.ru
Processing of personal data
































