




Contents
Scroll to:
https://doi.org/10.47093/2218-7332.2025.16.3.48-55
Scroll to:
One of the rare forms of anemia in patients with liver cirrhosis (LC) is acanthocytosis (spur cell anemia) – a non‑immune hemolytic anemia caused by alterations in the lipid composition of the red blood cells membrane because of severe liver failure.
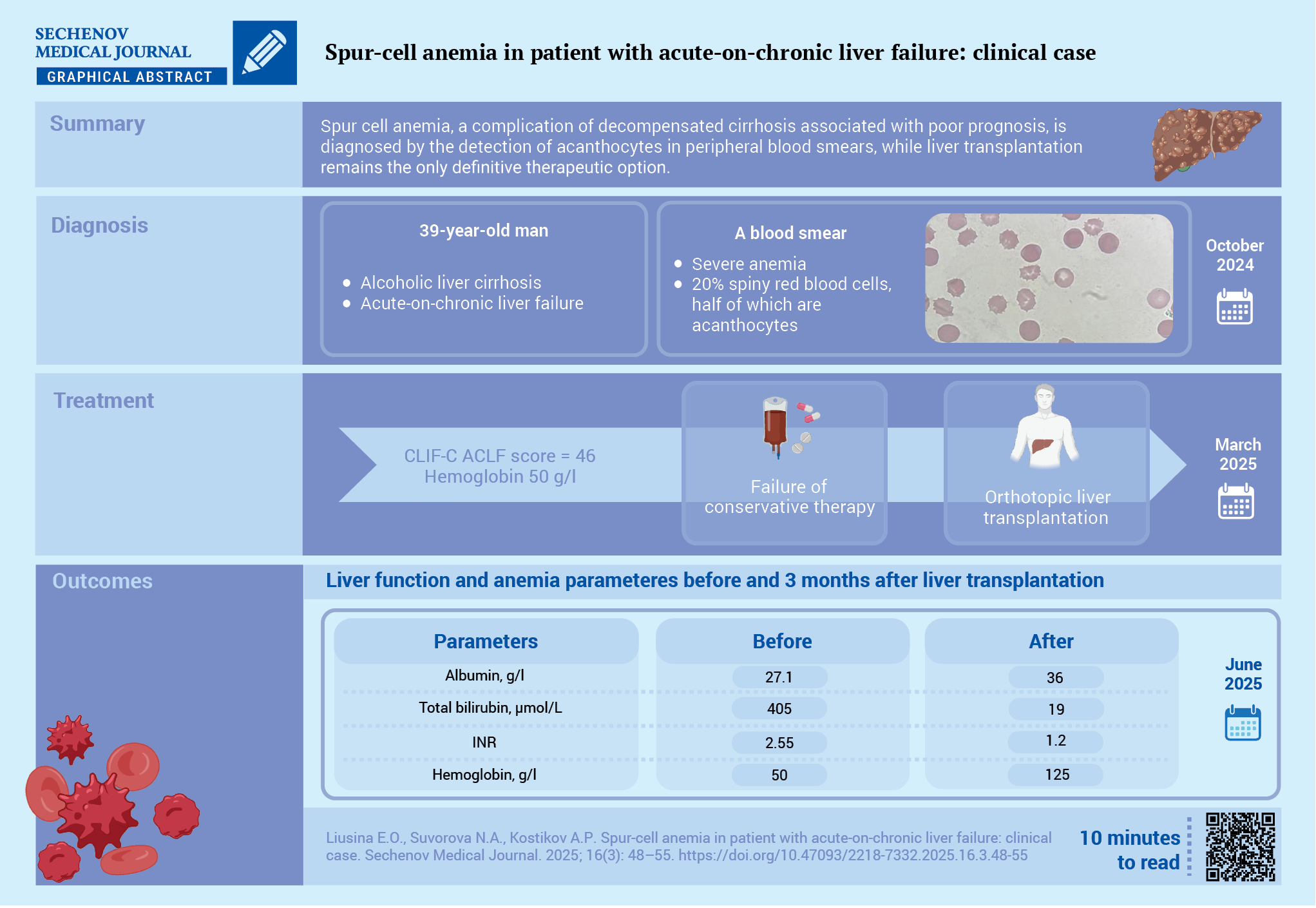
Case report. A 37‑year‑old patient with decompensated alcoholic LC (Child‑Pugh class C, the MELD‑Na (Model for End‑Stage Liver Disease – Na) score was 34 points) presented with severe weakness and dyspnea. Acute‑on‑chronic liver failure was diagnosed: CLIF‑C ACLF (Chronic Liver Failure Consortium Acute‑on‑Chronic Liver Failure Score) score was 46. Severe macrocytic anemia with reticulocytosis was detected: hemoglobin – 50 g/L, red blood cells – 1.26×10¹²/L, reticulocytes – 77.9 ‰. Other causes of anemia, such as blood loss, iron deficiency, vitamin B12 and folate deficiencies were excluded. The Coombs test was negative, and bone marrow examination ruled out myelodysplasia. Blood smear analysis revealed that 20% of red blood cells had the shape of spur cells, with approximately half of them being acanthocytes. Orthotopic liver transplantation was performed. Follow-up examination after three months showed normalization of liver function tests and absence of anemia and acanthocytosis.
Discussion. This case report highlights the need for blood smear examination to detect acanthocytes – a rare but prognostically unfavorable cause of anemia in patients with LC. Liver transplantation remains the only effective treatment option.
Anemia is a common complication of liver cirrhosis (LC), occurring in 66–75% of patients, and is associated with a higher rate of cirrhosis decompensation, hospital admissions, development of acute-on-chronic liver failure (ACLF), reduced survival, and increased mortality [1][2]. The most common etiological factors of anemia in LC patients are iron, folic acid, and vitamin B12 deficiencies, as well as chronic inflammation.
One of the least studied and rarely diagnosed forms of anemia in patients with LC is spur cell anemia (SCA) — a type of non-immune hemolytic anemia that develops because of abnormalities in the lipid composition of red blood cells membranes. In particular, there is an increase in the cholesterol-to-phospholipid and protein ratio, which in turn increases membrane rigidity, reduces its fluidity, and leads to mechanical damage of the cells. In addition, fatty acid metabolism is disrupted: their incorporation into phosphatidylethanolamine decreases, while incorporation into acylcarnitine increases. Such disturbances are characteristic of all forms of SCA, as they impair the restoration of membrane lipids and lead to the formation of characteristic protrusions (spurs) on the red blood cells surface, which can be observed under blood smear microscopy [3].
Spur-shaped red blood cells (acanthocytes) undergo hemolysis and are eliminated by the mononuclear phagocyte system. The standard diagnostic criterion for SCA is the detection of more than 5% acanthocytes in a blood smear with a hemoglobin level below 100 g/L and the exclusion of other causes of anemia [4].
The development of SCA in patients with LC is associated with an unfavorable prognosis, frequent episodes of decompensation, and higher mortality rates [5–7].
Currently there is no effective treatment for SCA; various pharmacological agents with different mechanisms of action and plasmapheresis have been described, although it is underlined that only liver transplantation leads to resolution of the anemia [8].
The aim of this case report is to demonstrate the development of secondary acanthocytosis in a patient with severe hepatic dysfunction and to increase clinicians’ awareness of this rare etiology of anemia.
A 37-year-old male patient, technical specialist with a history of alcohol abuse over the past 3–5 years first noted scleral icterus in November 2023. Laboratory tests revealed elevated levels of bilirubin, alanine aminotransferase, aspartate aminotransferase, and gamma-glutamyl transpeptidase. Viral and autoimmune etiologies of liver disease, Wilson’s disease, and hereditary haemochromatosis were excluded. The patient had no metabolic risk factors, and ultrasonography of the liver showed no signs of steatosis, which allowed the exclusion of metabolic dysfunction-associated steatotic liver disease. Upon alcohol abstinence, jaundice regressed.
In April 2024, the patient developed recurrent jaundice. Laboratory tests revealed hyperbilirubinemia, elevated alanine aminotransferase, aspartate aminotransferase, and gamma-glutamyl transpeptidase, hypoalbuminemia, moderate thrombocytopenia, and a slight decrease in hemoglobin to 121 g/L (Table). Imaging investigations showed signs of portal hypertension (grade 2 esophageal varices, minimal ascites, splenomegaly). A diagnosis of severe alcoholic hepatitis (Maddrey’s discriminant function was 41) and LC was established. The patient responded to treatment with prednisolone 40 mg/day: on the day 7th, the Lille score was 0.06, which after prednisolone was gradually tapered and discontinued. During therapy, the severity of jaundice decreased, although complete regression was not achieved.
Table. Dynamics of laboratory parameters in a patient with liver cirrhosis
|
Parameter |
Ref. range |
Nov. 2023 |
Apr. 2024 |
Aug. 2024 |
Oct. 2024 |
Jul. 2025 |
|
Complete Blood Count |
||||||
|
hemoglobin, g/l |
130–170 |
132 |
121 |
79 |
50 |
125 |
|
red blood cells, ×10¹²/l |
4.3–5.7 |
4.2 |
3.5 |
2.3 |
1.3 |
4.0 |
|
reticulocytes, ‰ |
77.9 |
5.1 |
||||
|
white blood cells, ×10⁹/l |
4.5–11.0 |
6.5 |
6.9 |
8.4 |
15.6 |
4.1 |
|
Neutrophils, ×10⁹/l |
1.78–5.38 |
5.2 |
11.1 |
2.0 |
||
|
Plateles, ×10⁹/l |
150–400 |
137 |
80 |
47 |
86 |
124 |
|
Biochemistry |
||||||
|
albumin, g/l |
35–52 |
31.2 |
27.6 |
27.1 |
36.0 |
|
|
ALT, U/l |
<35 |
80 |
58 |
27 |
13 |
12 |
|
AST, U/l |
<35 |
230 |
72 |
82 |
52 |
17 |
|
LDH, U/l |
671 |
182 |
||||
|
GGTP, U/l |
<49 |
938 |
526 |
621 |
749 |
32 |
|
total bilirubin, µmol/l |
3.4–20.5 |
42 |
214 |
273 |
405 |
|
|
direct bilirubin, µmol/l |
<8.6 |
34 |
176 |
207 |
172 |
|
|
creatinine, µmol/l |
49–90 |
70 |
95 |
110 |
152 |
127 |
|
cholesterol, mmol/l |
<5.0 |
6.7 |
2.5 |
1.9 |
3.2 |
|
|
C-reactive protein, mg/L |
<5.0 |
36 |
20 |
3 |
||
|
Coagulation panel |
||||||
|
INR |
0.8–1.2 |
1.13 |
1.75 |
1.65 |
2.55 |
1.20 |
|
prothrombin time, sec |
9.4–12.5 |
18.7 |
23.4 |
|||
|
fibrinogen, g/l |
2.0–4.0 |
3.1 |
2.6 |
1.5 |
1.8 |
2.4 |
Note: ALT – alanine aminotransferase; AST – aspartate aminotransferase; GGTP – gamma-glutamyltranspeptidase; INR – international normalized ratio; LDH – lactate dehydrogenase.
In August 2024, the patient’s condition deteriorated, with the onset of weakness, dyspnea, ascites, and oedema. Laboratory tests revealed hyperbilirubinemia, marked hypoalbuminemia, severe anemia (hemoglobin – 79 g/L), elevated C-reactive protein, and deficiencies of vitamin B12 (159 pg/mL) and folates (1.9 ng/mL) (Table). Iron metabolism indices were within the reference ranges. The severity of LC was classified as Child–Pugh C, MELD-Na (Model for End-Stage Liver Disease – Na) was 25 points. The anemia was initially attributed to vitamin B12 and folate deficiency. Treatment included albumin infusions, a single erythrocyte transfusion, spironolactone, furosemide, rifaximin, vitamin B12, folic acid, and thiamine. Improvement was observed, with reduction in oedema and ascites, some alleviation of weakness and dyspnea, and a transient increase in hemoglobin to 85 g/L.
During the following month, progressive weakness, dyspnea, and oedema recurred. The patient was readmitted in October 2024. On examination: body temperature 36.5 °C, oxygen saturation 98%, clear consciousness (Glasgow Coma Scale score was 15), no signs of overt hepatic encephalopathy. The skin, sclerae, and visible mucosae were icteric, lower extremities oedema were present. Heart rate was 83 bpm, blood pressure – 115/75 mmHg. The abdomen was enlarged due to non-tensed ascites, non-tender on palpation, hepatosplenomegaly was noted.
Abdominal ultrasound showed grade 2 ascites, hepatosplenomegaly, and dilation of the portal and splenic veins. Upper endoscopy showed grade 2 oesophageal varices.
Laboratory tests demonstrated persistent marked hyperbilirubinemia involving both fractions, elevated gamma-glutamyl transpeptidase, impaired hepatic protein-synthetic function (hypoproteinemia, hypoalbuminemia, hypocholesterolemia, hypocoagulation), elevated C-reactive protein, and increased creatinine up to 152 µmol/L.
A complete blood count revealed severe macrocytic anemia with reticulocytosis: hemoglobin – 50 g/L, red blood cells – 1.26×10¹²/L, reticulocytes – 77.9 ‰, MCV (mean corpuscular volume) – 126 fL; moderate thrombocytopenia (platelets – 86×10⁹/L), and leukocytosis (white blood cells – 15.6×10⁹/L) with a left shift (Table).
Urinalysis showed increased urobilinogen and direct bilirubin, but no free hemoglobin, proteinuria or urinary sediment abnormalities.
A diagnostic workup for the causes of anemia was conducted. Occult blood was not detected in stool samples (tested twice). Iron metabolism parameters — serum iron (26 µmol/L), transferrin saturation (47%), and latent iron-binding capacity (24.9 µmol/L) — were within reference limits, excluding iron deficiency. Serum vitamin B12 (201.4 pg/mL) and folic acid (9.2 ng/mL) concentrations were within normal ranges. Lactate dehydrogenase levels were elevated, and the direct Coombs test was negative.
A peripheral blood smear demonstrated anisocytosis (macrocytosis), poikilocytosis, spherocytes, target cells, and 20% of red blood cells with spur-like morphology, approximately half of which were acanthocytes. Howell–Jolly bodies were observed in some red blood cells (Figure). The patient was examined by a hematologist, and sternal puncture revealed erythroid hyperplasia. To exclude hypothyroidism as a potential cause of secondary acanthocytosis, thyroid-stimulating hormone was measured (2.5 mIU/L), which was within the reference range.

FIG. Peripheral blood smear, Romanowsky–Giemsa stain, magnification ×1000.
Note: 1 – normal red blood cell; 2 – pathological red blood cell inclusions (Howell–Jolly bodies); 3 – spherocyte; 4 – target cell; 5 – spur cell: echinocyte (uniform, evenly distributed spicules); 6 – spur cell: acanthocyte (irregular, unevenly distributed spicules).
Thus, in a patient with toxic etiology liver cirrhosis (Child–Pugh class C, MELD-Na was 34), ACLF was diagnosed: CLIF-C ACLF (Chronic Liver Failure Consortium Acute-on-Chronic Liver Failure score)1 score was 46. The severity of ACLF was grade 2 with the development of hepatic failure and acute kidney injury of prerenal origin stage 1 according to KDIGO (Kidney Disease: Improving Global Outcomes). Based on hematological evaluation, secondary acanthocytosis was diagnosed in the patient with severe hepatic failure.
Treatment of LC and its complications was conducted in accordance with the clinical guidelines of the Ministry of Health of the Russian Federation2. To correct anemia, three packed red blood cell transfusions were performed, achieving a maximum hemoglobin level of 71 g/L.
The patient met the criteria for severe decompensated LC with signs of poor prognosis, which justified consultation with a transplant specialist and placement on the liver transplantation waiting list. In spring 2025, orthotopic liver transplantation was performed. The surgical procedure was completed without complications, appropriate immunosuppressive therapy was administered, and three months post-transplantation, anemia resolved: hemoglobin was 125 g/L, red blood cells – 4.0×10¹²/L, and no acanthocytes were detected (Table).
Approximately in 50% of anemia cases observed in patients with liver cirrhosis, as reported by B. Scheiner et al. [1], the underlying etiology remains unknown even after comprehensive laboratory and instrumental diagnostic work up.
The presented clinical case shows the diagnostic workup for anemia, during which all causes of anemia (iron-deficiency, megaloblastic, and hemolytic anemias (including autoimmune anemia and anemia associated with Wilson’s disease), as well as anemia due to bone marrow aplasia) were excluded. Based on the combination of clinical, laboratory, and morphological data, a diagnosis of secondary acanthocytosis due to LC was established. Another potential mechanism contributing to anemia could be chronic inflammation in the patient with LC; however, iron metabolism parameters did not indicate functional iron deficiency.
Microscopic examination of the peripheral blood smear revealed diverse red blood cells morphologies: hyperchromic macrocytes, spherocytes, codocytes, echinocytes, acanthocytes, and red blood cells containing Howell–Jolly bodies. This combination may reflect both the severity of the underlying disease and the effects of therapeutic interventions. The presence of spherocytes is likely related to prior blood transfusions, while Howell–Jolly bodies and pronounced poikilocytosis indicate functional hyposplenism developing in LC and during hemolysis [9].
In this case, the absence of hematological pathology prior to liver disease manifestation excludes hereditary forms of acanthocytosis. Normal thyroid-stimulating hormone levels and bone marrow findings ruled out hypothyroidism and myelodysplasia as causes of secondary acanthocytosis.
In routine clinical practice, distinguishing acanthocytes from echinocytes in blood smears may present certain diagnostic challenges. Acanthocytes are pathological, irreversibly altered red blood cells with unevenly distributed spicules, formed due to lipid metabolism disorders, membrane damage from hemolysis, and impaired splenic clearance of defective red blood cells [10]. Echinocytes, by contrast, have evenly distributed projections and are reversible; their appearance may result from osmolarity disturbances, smear preparation technique, or sample transport [11].
SCA in patients with alcoholic LC must be differentiated from Zieve’s syndrome, which presents with the triad of hemolysis, jaundice, and dyslipidemia. In Zieve’s syndrome, improvement may occur with alcohol cessation and conservative therapy, whereas SCA is irreversible and serves as a marker of poor prognosis [12], as observed in the presented case.
Pharmacotherapy for SCA remains insufficiently studied: few case reports describe positive effects of flunarizine, pentoxifylline, cholestyramine, high-dose steroids, and plasmapheresis [2][13][14]. Blood transfusions provide temporary correction but may contribute to iron overload and progression of liver damage.
In the presented patient, the development of ACLF and secondary acanthocytosis were extremely poor prognostic factors. It should be emphasized that among all available interventions, only liver transplantation has demonstrated the ability to reverse both hepatic decompensation and the characteristic red blood cells changes observed in acanthocytosis [15]. This was clearly illustrated by the outcome in our patient.
Given the high prognostic significance of acanthocytosis even in the absence of anemia in patients with ACLF [7], it can be anticipated that this parameter may be evaluated for potential inclusion in future ACLF severity scoring systems.
The presented clinical case of SCA highlights the complexity of diagnosing rare causes of anemia in patients with decompensated LC and ACLF. Morphological assessment of peripheral blood smears is a simple and accessible method for detecting acanthocytosis. Liver transplantation remains the only intervention capable of achieving regression of both hepatic insufficiency and acanthocytosis.
Ekaterina O. Liusina, Natalia A. Suvorova and Andrey P. Kostikov participated in the examination, treatment of the patient, literature analysis, preparation of the manuscript text, and critical revision of the manuscript. All the authors approved the final version of the article.
Compliance with ethical standards. Consent statement. The patient consented to the publication of the article “Spur-cell anemia in patient with acute-on-chronic liver failure: clinical case” in the “Sechenov Medical Journal”.
Conflict of interests. The authors declare that there is no conflict of interest.
Financing. The study had no sponsorship (own resources).
Acknowledgments. The authors express their deep gratitude to the Doctor of Clinical Laboratory diagnostics Tatyana V. Dudik (City Clinical Hospital No. 15 named after O.M. Filatov) for the photographs of the micropreparation provided; to physician Dayana A. Fedorova (City Clinical Hospital No. 15 named after O.M. Filatov), to Head of the Hepatology Department Ekaterina E. Starostina (E.M. Tareev Clinic of Rheumatology, Nephrology, and Occupational Pathology Sechenov First Moscow State Medical University (Sechenov University)), and to gastroenterologist-hepatologist Igor N. Tikhonov (V. Kh. Vasilenko Clinic of Internal Disease Propaedeutics, Gastroenterology and Hepatology Sechenov First Moscow State Medical University (Sechenov University)) for assistance in collecting clinical material and documenting observations.
1. Chronic Liver Failure Consortium Acute-on-Chronic Liver Failure score. https://efclif.com/research-infrastructure/score-calculators/clif-c-of-aclf-ad/ (access date: 05.06.2025).
2. Ministry of Health of the Russian Federation. Clinical Guidelines. Liver Cirrhosis and Fibrosis (approved by the Ministry of Health of the Russian Federation, 2022) https://cr.minzdrav.gov.ru/view-cr/715_2 (access date: 05.06.2025).
1. Scheiner B., Semmler G., Maurer F., et al. Prevalence of and risk factors for anaemia in patients with advanced chronic liver disease. Liver Int. 2020 Jan; 40(1): 194–204. https://doi.org/10.1111/liv.14229. PMID: 31444993
2. Gonzalez-Casas R., Jones E.A., Moreno-Otero R. Spectrum of anemia associated with chronic liver disease. World J Gastroenterol. 2009 Oct; 15(37): 4653–4658. https://doi.org/10.3748/wjg.15.4653. PMID: 19787828
3. Sharma R., Holman C.J., Brown K.E. A thorny matter: Spur cell anemia. Ann Hepatol. 2023 Jan-Feb; 28(1): 100771. https://doi.org/10.1016/j.aohep.2022.100771. Epub 2022 Oct 12. PMID: 36241039
4. Roy A., Rodge G., Goenka M.K. Spur Cell Anaemia in Cirrhosis: A Narrative Review. J Clin Exp Hepatol. 2023 May-Jun; 13(3): 500–508. https://doi.org/10.1016/j.jceh.2022.10.005. Epub 2022 Oct 11. PMID: 37250881
5. Virk Z.M., Patel A.A., Leaf R.K., Al-Samkari H. Predictors of mortality and outcomes of liver transplant in spur cell hemolytic anemia. Am J Hematol. 2021 Dec; 96(12): 1611–1620. https://doi.org/10.1002/ajh.26359. Epub 2021 Oct 7. PMID: 34553418
6. Alexopoulou A., Vasilieva L., Kanellopoulou T., et al. Presence of spur cells as a highly predictive factor of mortality in patients with cirrhosis. J Gastroenterol Hepatol. 2014 Apr; 29(4): 830–834. https://doi.org/10.1111/jgh.12473. PMID: 24325340
7. Bevilacqua M., De Marco L., Stupia R., et al. Spur cells in liver cirrhosis are predictive of acute-on-chronic liver failure and liverrelated mortality regardless of severe anaemia. Intern Emerg Med. 2023 Aug; 18(5): 1397–1404. https://doi.org/10.1007/s11739-023-03303-x. Epub 2023 May 22. PMID: 37212944
8. Katiyar V., Dadlani A., Vohra I., et al. An Unusual Case of Hemolytic Anemia Reversed with Liver Transplantation. Int J Hematol Oncol Stem Cell Res. 2022 Apr; 16(2): 128–130. https://doi.org/10.18502/ijhoscr.v16i2.9206. PMID: 36304733
9. Fierro-Angulo O.M., González-Regueiro J.A., Pereira-García A., et al. Hematological abnormalities in liver cirrhosis. World J Hepatol. 2024 Sep; 16(9): 1229–1244. https://doi.org/10.4254/wjh.v16.i9.1229. PMID: 39351511
10. Perrin J., Georges A., Morali A., et al. Acanthocytes et hypocholestérolémie [Acanthocytes and hypocholesterolemia]. Ann Biol Clin (Paris). 2008 Sep-Oct; 66(5): 569–572. French. https://doi.org/10.1684/abc.2008.0269. PMID: 18957348
11. Foglia A. The acanthocyte-echinocyte differential: The example of chorea-acanthocytosis. Swiss Med Wkly. 2010 Jul; 140: 10.4414/ smw.2010.13039. https://doi.org/10.4414/smw.2010.13039. PMID: 20131113
12. Ribeiro R., Ferreira M., Coelho R., Pereira C. Zieve’s Syndrome: An Underdiagnosed Cause of Non-immune Hemolytic Anemia. Cureus. 2024 Jan; 16(1): e52034. https://doi.org/10.7759/cureus.52034. PMID: 38344483
13. Aihara K., Azuma H., Ikeda Y., et al. Successful combination therapy—flunarizine, pentoxifylline, and cholestyramine—for spur cell anemia. Int J Hematol. 2001 Apr; 73(3): 351–355. https://doi.org/10.1007/bf02981961. PMID: 11345202
14. Miki K., Maruki T., Imashuku S. Plasmapheresis for Spur Cell Anemia in a Patient with Alcoholic Liver Cirrhosis. Case Rep Hematol. 2018 Jun; 2018: 9513946. https://doi.org/10.1155/2018/9513946. PMID: 30034891
15. Piano S., Tonon M., Vettore E., et al. Incidence, predictors and outcomes of acute-on-chronic liver failure in outpatients with cirrhosis. J Hepatol. 2017 Dec; 67(6): 1177–1184. https://doi.org/10.1016
Ekaterina O. Liusina, Cand. of Sci. (Medicine), Research Associate, Laboratory of Experimental and Preventive Gastroenterology, National Medical Research Center for Therapy and Preventive Medicine; gastroenterologist, LLC “Chaika White Gardens”.
10/3, Petroverigsky Ln., Moscow, 101990,
9, Lesnaya str., Moscow, 125196
Natalia A. Suvorova, Cand. of Sci. (Medicine), Associate Professor, Department of Hospital Therapy named after Academician P.E. Lukomsky, Pirogov Russian National Research Medical University; physician, City Clinical Hospital No. 15 named after O.M. Filatov; gastroenterologist, LLC “DOCMED”
1/6, Ostrovityanova str., Moscow, 117513,
23, Veshnyakovskaya str., Moscow, 111539,
35, Trubnaya str., Moscow, 127051
Andrey P. Kostikov, physician
21, Palekhskaya str., Moscow, 129337

|
1. CARE checklist | |
| Subject | ||
| Type | Исследовательские инструменты | |
Download
(424KB)
|
Indexing metadata ▾ | |
Sechenov Medical Journal. Editor's checklist for this article you can find here.
Журнал «Сеченовский вестник» |
| Sechenov Medical Journal |
Рецензии на рукопись |
| Peer-review reports |
Название / Title | Акантоцитоз – редкая причина анемии у пациента с острым повреждением печени на фоне хронического: клинический случай / Spur-cell anemia in patient with acute-on-chronic liver failure: clinical case
|
Раздел / Section
| ВНУТРЕННИЕ БОЛЕЗНИ / INTERNAL DISEASES
|
Тип / Article | Клинический случай / Сlinical case |
Номер / Number | 1342
|
Страна/территория / Country/Territory of origin | Россия / Russia |
Язык / Language | Английский / English
|
Источник / Manuscript source | Инициативная рукопись / Unsolicited manuscript |
Дата поступления / Received | 15.08.2025
|
Тип рецензирования / Type ofpeer-review | Двойное слепое / Double blind |
Язык рецензирования / Peer-review language | Английский /Русский/ English /Russian |
РЕЦЕНЗЕНТ А / REVIEWER A
Инициалы / Initials | 1342_А
|
Научная степень / Scientific degree | Кандидат медицинских наук / Cand. of Sci. (Medicine)
|
Страна/территория / Country/Territory | Россия / Russia
|
Дата рецензирования / Date of peer-review | 08.09.2025 |
Число раундов рецензирования / Number of peer-review rounds | 1 |
Финальное решение / Final decision | принять к публикации после небольшой доработки/ minor revision
|
ПЕРВЫЙ РАУНД РЕЦЕНЗИРОВАНИЯ / FIRST ROUND OF PEER-REVIEW
Статья представляет большой интерес для практикующих врачей-гастроэнтерологов, способствует расширению знаний в смежных областях (гематология) и рекомендуется к публикации в журнале.
Однако, целесообразно обратить внимание на отдельные замечания.
ЗАКЛЮЧЕНИЕ: принять к публикации после небольшой доработки.
РЕЦЕНЗЕНТ B / REVIEWER B
Инициалы / Initials | 1342_В
|
Научная степень / Scientific degree | Кандидат медицинских наук / Cand. of Sci. (Medicine) |
Страна/территория / Country/Territory | Россия/ Russia
|
Дата рецензирования / Date of peer-review | 06.09.2025 |
Число раундов рецензирования / Number of peer-review rounds | 1 |
Финальное решение / Final decision | принять к публикации / accept
|
ПЕРВЫЙ РАУНД РЕЦЕНЗИРОВАНИЯ / FIRST ROUND OF PEER-REVIEW
Описание клинического случая шпороклеточной анемии у пациента с циррозом печени несомненно представляет большой научный и практический интерес, какдля аудитории врачей-гастроэнтерологов, так и для специалистов-гематологов.
Установленный диагноз не вызывает сомнений, представленный алгоритм дифференциальной диагностики анемии обоснован и включает все необходимые исследования для исключения альтернативных причин анемии в данной клинической ситуации.
Принципиальные замечания к статье отсутствуют.
Предложения:
1) препарат Сульцеф указан по торговому наименованию, необходимо исправить на МНН;
2) предлагается добавить более полное описание миелограммы (представить эритродный росток в процентах, описать морфологические особенности клеток, представить фотографию миелограммы);
3) отсутствуют значения ЛДГ - важного маркера внутрисосудистого гемолиза, а также гаптоглобина (не обязательно, но желательно).
ЗАКЛЮЧЕНИЕ: принять к публикации.
РЕКОМЕНДАЦИИ НАУЧНЫХ РЕДАКТОРОВ ЖУРНАЛА / RECOMMENDATIONS
OF THE SCIENTIFIC EDITORS OF THE JOURNAL
Метаданные
Основной текст
Рисунки
Рисунок 1 прислать в хорошем качестве отдельным файлом.
Список литературы
(раздел 5.7
https://www.sechenovmedj.com/jour/about/submissions#authorGuidelines )
Согласия
Графический абстракт
Для оптимизации времени подготовки статьи просим авторов начать готовить графический абстракт на русском и на английском языке. Шаблон графического абстракта можно найти в начале раздела "Правила для авторов"
https://www.sechenovmedj.com/jour/about/submissions#authorGuidelines .

8-2 Trubetskaya st., Moscow, 119048
Federal State Autonomous Educational Institution of Нigher Education I.M.Sechenov First Moscow State Medical University of the Ministry of Health of the Russian Federation (Sechenovskiy University)
E-mail: sechenovmedj@staff.sechenov.ru
Processing of personal data
































