



Contents
Scroll to:
 M. G. Chashchin,
Z. I. Khutaeva,
G. A. Konovalov,
M. B. Mukhtarov,
Z. M. Musaeva,
Kh. A. Khashieva,
V. L. Averkiev,
V. S. Rabicheva,
A. Yu. Gorshkov,
O. M. Drapkina
M. G. Chashchin,
Z. I. Khutaeva,
G. A. Konovalov,
M. B. Mukhtarov,
Z. M. Musaeva,
Kh. A. Khashieva,
V. L. Averkiev,
V. S. Rabicheva,
A. Yu. Gorshkov,
O. M. Drapkina https://doi.org/10.47093/2218-7332.2026.17.1.4-17
Scroll to:
Lipoprotein (a) (Lp(a)) is a genetically determined risk factor for atherosclerosis, with extremely high levels associated with very high cardiovascular risk. Despite this, in routine clinical practice these patients often remain insufficiently identified.
Aim. To characterize the prevalence and severity of subclinical atherosclerosis in various vascular beds in patients with Lp(a) ≥ 180 mg/dL, including younger age groups.
Materials and methods. We performed a retrospective analysis of a database comprising 101,078 outpatients, from which 1105 (1.09%) individuals with Lp(a) ≥ 180 mg/dL and available lipid profile data were selected; women accounted for 67.2%, and the mean age was 52.74 ± 14.59 years. The presence of atherosclerotic cardiovascular disease (ASCVD) was ascertained from medical records, and atherosclerosis was assessed by duplex ultrasound of the brachiocephalic arteries (BCA) and lower extremity arteries (LEA), as well as by the Agatston coronary artery calcium score (CACS). At least one vascular bed was evaluated in 69.8% of patients, and all three were evaluated in 6.2%.
Results. Most patients showed elevated levels of total cholesterol and low-density lipoprotein cholesterol. From the age of 25–44 years onward, a substantial proportion of patients already showed atherosclerotic involvement of the BCA and LEA with stenosis ≥20% and pronounced coronary calcification (CACS > 100 units), with a shift toward more severe lesions in older age groups. In the subgroup that underwent imaging of all three vascular beds, 60.0% of patients aged 25–44 years had two or three beds that were affected; the proportion of patients with involvement of all three vascular beds increased to 40.0% in those aged 45–59 years, 76.9% in those aged 60–74 years, and reached 100% in patients aged ≥ 75 years (p < 0.001). The prevalence of clinically documented ASCVD increased from 10.3% in the 25–44 age group to 67.1% in patients aged ≥ 75 years. Even among patients without documented ASCVD, atherosclerotic involvement of the BCA, LEA and coronary calcification was detected in 85.9%, 82.6% and 37.1% of cases, respectively.
Conclusion. Patients with Lp(a) ≥ 180 mg/dL are characterized by a high prevalence and early onset of subclinical, frequently multifocal atherosclerosis, with a pronounced age-related gradient of progression. These findings support the case for designating this cohort as a priority group for in-depth evaluation, risk re-stratification and more intensive preventive management.
Lipoprotein (a) (Lp(a)) is a genetically determined risk factor for atherosclerotic cardiovascular disease (ASCVD). Plasma Lp(a) concentration is largely genetically determined, reaches stable values in early childhood, and remains essentially constant throughout life.
Elevated Lp(a) is detected in approximately 20% of the general population and represents one of the most common inherited dyslipidemias [1]. Current clinical guidelines and consensus statements recommend a one-time measurement of Lp(a) in every adult. In real-world practice, however, the testing rate remains very low (less than 1%) and does not reflect the epidemiological importance of this risk factor [2–5].
Particular clinical interest is drawn to patients with Lp(a) ≥ 180 mg/dL (≥430 nmol/L), which corresponds to approximately the 99th percentile of the population distribution and affects roughly 1% of the population (about 1 in 100 individuals) – nearly three times more frequently than heterozygous familial hypercholesterolemia (around 1:313) [6][7]. In terms of prognostic significance for cardiovascular outcomes, extremely high Lp(a) is comparable to classical forms of inherited dyslipidemia, primarily familial hypercholesterolemia. Despite this, patients with extremely high Lp(a) remain underrepresented in clinical research and, in particular, poorly characterized in routine clinical settings, including with respect to detection rates, clinical and demographic profile, ASCVD burden, and the specifics of preventive and therapeutic strategies.
Epidemiological and genetic studies show that as Lp(a) levels rise, the risk of ASCVD progressively increases, the spectrum of associated vascular lesions broadens, and a pan-vascular pattern of involvement emerges. In a large population-based study, Lp(a) above the 95th percentile (≥120 mg/dL) was associated with an almost 4-fold increase in the risk of a first myocardial infarction [8]. In another large prospective study, Lp(a) values above the 99th percentile (≥143 mg/dL) were associated with a 2- to 3-fold increase in the risk of peripheral artery disease and abdominal aortic aneurysm [9].
A pooled analysis of Danish cohorts demonstrated that Lp(a) above the 95th percentile (>90 mg/dL) was associated with an almost 3-fold increase in the risk of degenerative aortic stenosis [10], and a 30-year follow-up of initially healthy women revealed significant associations between high Lp(a) concentrations and the risk of ischemic stroke and cardiovascular mortality [11].
Together, these data emphasize that early identification of elevated Lp(a) is critically important not only in the context of coronary risk, but also with respect to a broader spectrum of vascular outcomes. Despite this, the real-world healthcare system still lacks a unified approach to the identification, evaluation and management of patients with extremely high Lp(a): testing is performed sporadically, referral pathways and the scope of additional work-up remain heterogeneous, and subclinical stages of atherosclerosis often go unrecognized despite their high prevalence. At the same time, this very category of patients is potentially highly amenable to proactive management through earlier and more intensive correction of modifiable risk factors and, in the longer term, the introduction of Lp(a)-targeted therapy.
In this context, organized screening programs become particularly important. Beginning in 2026, the Russian Federation’s medical examination (dispanserization) program includes a one-time laboratory measurement of Lp(a) in individuals aged 18–40 years1. Indications for testing include a family history of cardiovascular disease, early-onset myocardial infarction or stroke, and a high cardiovascular risk despite normal low-density lipoprotein cholesterol (LDL-C). Patients with elevated Lp(a), particularly those with extreme values, require subsequent follow-up and the application of personalized diagnostic and preventive algorithms.
The aim of the study was to provide a comprehensive evaluation of the lipid profile and the prevalence and pattern of clinical and subclinical atherosclerosis across several vascular beds in patients with extremely high Lp(a) ≥ 180 mg/dL, and to determine its relevance for cardiovascular risk stratification.
A retrospective analysis of real-world clinical data was performed. Electronic medical records of patients undergoing outpatient evaluation at the MEDSI Group clinics (Moscow and the Moscow Region) between January 5, 2022, and May 29, 2025 were reviewed. Prior to analysis, all personal data were anonymized in accordance with current legislation and internal regulations on the protection of medical information.
The source database comprised 101,078 patients in whom Lp(a) had been measured as part of routine clinical practice. From this sample, patients with Lp(a) ≥ 180 mg/dL and available lipid profile parameters – total cholesterol (TC), LDL-C, high-density lipoprotein cholesterol (HDL-C) and triglycerides (TG) – were selected. The final study cohort consisted of 1105 patients (1.09% of the total database) who were not receiving therapeutic apheresis.
Demographic variables included age and sex. Patients were stratified by age according to the following categories: under 18 years – children and adolescents; 18–24 years – young adults; 25–44 years – early adulthood; 45–59 years – middle age; 60–74 years – older age; and 75 years and over – advanced age.
History of myocardial infarction or ischemic stroke, coronary interventions (coronary stenting, coronary artery bypass grafting), the presence of coronary artery disease (CAD), as well as ASCVD risk factors (arterial hypertension, type 2 diabetes mellitus, smoking) were recorded on the basis of the documented diagnosis in the medical record.
A positive family history was recorded when there was documentation of CAD, stroke or hypercholesterolemia in first-degree relatives.
Laboratory analyses were performed in the certified laboratory of the MEDSI Group network in accordance with internal quality control standards and participation in an external quality assessment scheme (EQAS). Venous blood was collected after an overnight fast. Lp(a) was measured by an immunoturbidimetric method with latex enhancement using monospecific antibodies to apolipoprotein (a) on a Beckman Coulter DxC 700 AU automated biochemistry analyzer (Beckman Coulter, USA). Lipid profile parameters were measured on the same analyzer using standard enzymatic-colorimetric and immunonephelometric methods.
Atherosclerotic involvement of three vascular beds was assessed by duplex ultrasound of the brachiocephalic arteries (BCA) and lower extremity arteries (LEA), as well as by non-contrast computed tomography with calculation of the coronary artery calcium score (CACS) by the Agatston method on a SOMATOM Definition AS scanner (Siemens Healthineers, Germany). For the BCA and LEA, the presence of atherosclerotic plaques and the maximum degree of stenosis according to the European Carotid Surgery Trial (ECST) criteria were recorded. CACS values were classified as 0, 1–10, 11–100, 101–399 and ≥ 400 units [3].
Data on the assessment of vascular beds (BCA, LEA, CACS) were available for 69.8% of patients (n = 771). One vascular bed had been imaged in 30.8% of patients (n = 340), two in 32.9% (n = 363), whereas evaluation of all three vascular beds had been performed in only 6.2% of patients (n = 68).
Normality of continuous variables was assessed using the Kolmogorov–Smirnov test with Lilliefors correction. Normally distributed continuous variables were summarized as mean and standard deviation (M ± SD), and non-normally distributed variables as median and interquartile range (Me [ Q25; Q75]).
Categorical variables were presented as absolute (n) and relative (%) frequencies. Comparisons of continuous variables among three or more groups were performed using the non-parametric Kruskal–Wallis test (H-statistic), with post-hoc pairwise comparisons performed using the Dunn test with Bonferroni correction. Comparisons of categorical variables among groups were performed using the Pearson χ² test. A two-sided p-value of < 0.05 was considered statistically significant.
Statistical analysis was performed using MedStat.Pro, version 0.8.1 (School of Medical Statistics, Moscow, Russia)2.
Women predominated in the study cohort: 67.2% (n = 743) versus 32.8% men (n = 362), corresponding to a sex ratio of approximately 2:1.
Patient age ranged from 6 to 94 years, with a mean of 52.74 ± 14.59 years. The bulk of the cohort consisted of patients of working age and early older age.
The age and sex distribution is presented in Figure 1. In the under-18 group, women accounted for 58.3%, and in the 18–24 age group, all eight patients were women. Among patients aged 25–44 years, women accounted for 53.3%, rising to 68.5% in the 45–59 age group and to 74.6% in the 60–74 age group. The highest proportion of women was observed in patients aged 75 years and over, where it reached 88.6%.
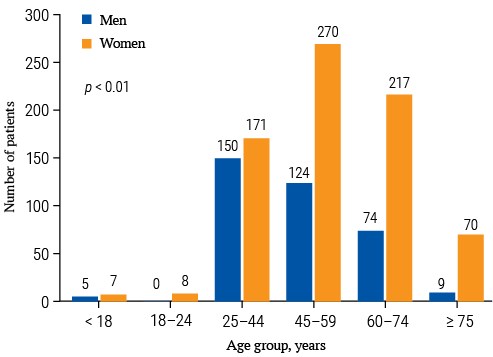
FIG. 1. Age and sex distribution of patients with extremely high lipoprotein (a) (n = 1105).
The cohort was heterogeneous: 779 patients (70.5%) had no history of documented ASCVD, whereas 326 (29.5%) had documented ASCVD. The proportion of patients with such events was 10.3% in those aged 25–44 years and rose progressively in older age groups, reaching 67.1% in patients aged 75 years and over (Fig. 2).
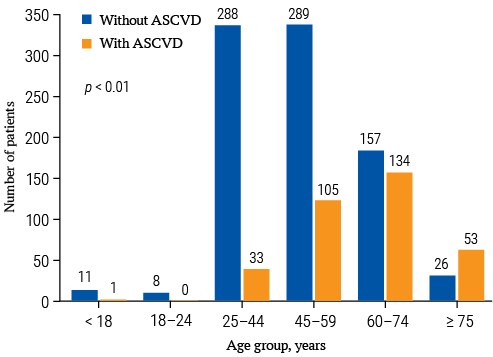
FIG. 2. Distribution of patients with extremely high lipoprotein (a) by history of atherosclerotic cardiovascular disease (n = 1105).
Note: ASCVD – atherosclerotic cardiovascular disease.
Of the documented ASCVD events, myocardial infarction was the most frequent: its prevalence increased approximately 10-fold when comparing patients aged 25–44 years with those aged 75 years and over. With increasing age, statistically significant increases were also observed for CAD, prior coronary interventions, type 2 diabetes mellitus and arterial hypertension. Already in the youngest adult group (25–44 years), CAD was present in 7.2% of patients, type 2 diabetes mellitus in 6.5%, arterial hypertension in 44.2%, and smoking in 38.9%; coronary artery bypass grafting had been performed in one patient. With advancing age, the frequency of CAD and myocardial revascularization rose further. The trajectory of ischemic stroke was similar: its prevalence increased approximately seven-fold in the oldest as compared with the youngest patients (Table 1).
Table 1. History of atherosclerotic cardiovascular disease in patients with extremely high lipoprotein (a) by age groups
|
History |
Age group |
p-value |
|||||
|
<18 (n = 12) |
18–24 (n = 8) |
25–44 (n = 321) |
45–59 (n = 394) |
60–74 (n = 291) |
≥75 (n = 79) |
||
|
Diseases: |
|||||||
|
myocardial infarction |
0 (0) |
0 (0) |
11 (3.4) |
65 (16.5) |
75 (25.8) |
27 (34.2) |
<0.001 |
|
ischemic stroke |
1 (8.3) |
0 (0) |
6 (1.9) |
18 (4.6) |
18 (6.2) |
12 (15.2) |
<0.001 |
|
CAD |
0 (0) |
0 (0) |
23 (7.2) |
87 (22.1) |
115 (39.5) |
47 (59.5) |
<0.001 |
|
Interventions: |
|||||||
|
coronary stenting |
0 (0) |
0 (0) |
0 (0) |
14 (3.6) |
19 (6.6) |
9 (11.4) |
<0.001 |
|
CABG |
0 (0) |
0 (0) |
1 (0.3) |
5 (1.3) |
11 (3.8) |
2 (2.5) |
0.032 |
|
Risk factors: |
|||||||
|
type 2 diabetes mellitus |
0 (0) |
0 (0) |
21 (6.5) |
63 (16.0) |
50 (17.2) |
29 (36.7) |
<0.001 |
|
arterial hypertension |
1 (8.3) |
0 (0) |
142 (44.2) |
281 (71.5) |
220 (75.6) |
65 (82.3) |
<0.001 |
|
smoking |
0 (0) |
0 (0) |
125 (38.9) |
162 (41.4) |
107 (36.9) |
15 (19.0) |
<0.001 |
|
Conditions in FDR: |
|||||||
|
CAD |
0 (0) |
1 (12.5) |
50 (15.6) |
80 (20.3) |
28 (9.6) |
4 (5.1) |
<0.001 |
|
ischemic stroke |
0 (0) |
0 (0) |
37 (11.5) |
61 (15.5) |
25 (8.6) |
3 (3.8) |
<0.001 |
|
hypercholesterolemia |
0 (0) |
1 (12.5) |
23 (7.2) |
22 (5.6) |
6 (2.1) |
1 (1.3) |
0.023 |
Notes: data are presented as the absolute number of patients with the characteristic and the proportion within the group, expressed as a percentage (in parentheses).
CABG – coronary artery bypass grafting; CAD – coronary artery disease; FDR – first-degree relatives.
A family history of CAD, stroke and hypercholesterolemia, by contrast, was more frequently reported by patients in younger and middle-aged groups, with a downward trend in older age groups.
Lp(a) concentration remained relatively stable across age groups, although between-group differences were statistically significant (p < 0.001). A modest increase in mean values was observed in the 45–59 and 60–74 age groups, but it did not give rise to clinically distinct subgroups. In patients aged 75 years and over, Lp(a) levels remained comparable to those in younger age groups (Table 2).
Table 2. Lipid profile in patients with extremely high lipoprotein (a) by age groups
|
Parameter |
Age group |
p-value |
|||||
|
<18 (n = 12) |
18–24 (n = 8) |
25–44 (n = 321) |
45–59 (n = 394) |
60–74 (n = 291) |
≥75 (n = 79) |
||
|
Lp(a), mg/dL |
198.92 ± 18.98 |
205.38 ± 40.17 |
204.45 ± 29.92b,c |
214.71 ± 45.65 |
219.07 ± 48.74 |
210.91 ± 37.74 |
<0.001 |
|
TC, mmol/L |
5.52 ± 0.85a,c |
6.31 ± 1.26 |
6.91 ± 1.28d |
7.02 ± 1.49d |
6.75 ± 2.01d |
5.59 ± 1.48 |
<0.001 |
|
TG, mmol/L |
0.96 ± 0.31b |
0.87 ± 0.32 |
1.48 ± 0.76b |
1.72 ± 0.97 |
1.66 ± 0.83 |
1.45 ± 0.48 |
<0.001 |
|
HDL-C, mmol/L |
1.50 ± 0.52 |
1.78 ± 0.27 |
1.61 ± 0.38 |
1.68 ± 0.40 |
1.68 ± 0.45 |
1.55 ± 0.34 |
0.022 |
|
LDL-C, mmol/L |
3.38 ± 0.60a,b |
3.93 ± 0.94 |
4.42 ± 0.95d |
4.46 ± 1.10d |
4.29 ± 1.39d |
3.39 ± 1.16 |
<0.001 |
Notes: superscript letters indicate statistically significant differences in post-hoc pairwise comparisons (Dunn test with Bonferroni correction): a p < 0.05 vs. 25–44 group; b p < 0.05 vs. 45–59 group; c p < 0.05 vs. 60–74 group; d p < 0.01 vs. ≥ 75 group.
HDL-C – high-density lipoprotein cholesterol; LDL-C – low-density lipoprotein cholesterol; Lp(a) – lipoprotein (a); TC – total cholesterol; TG – triglycerides.
Analysis of the distribution of Lp(a) values showed that older age groups were characterized not by a shift in central tendency, but by greater variability driven by the appearance of isolated extreme values (Supplementary materials on the journal’s website https://doi.org/10.47093/2218-7332.2026.17.1.4-17-annex). At the same time, baseline Lp(a) levels remained consistently high regardless of age, in keeping with the genetically determined nature of this trait.
Most patients had elevated TC and LDL-C levels, reflecting a markedly atherogenic background in the study cohort (Table 2). The highest TC and LDL-C levels were observed in patients aged 25–59 years, with an upward trend already apparent from the 18–24 age group. In older age groups (≥60 years), TC and LDL-C tended to decline relative to the 25–59-year peak, although values remained elevated.
TG concentrations showed a moderate increase predominantly in the 25–59 age range, followed by a decline in older age groups. HDL-C remained relatively stable across age subgroups, with only modest differences that were not statistically significant in pairwise comparisons.
Duplex ultrasound of the BCA was available for 66.2% (n = 731) of patients. Moderate stenoses (20–34%) predominated and were identified in 67.9% of patients. Mild stenoses (< 20%) were much less common (11.6%), whereas hemodynamically significant stenoses (>55%) were detected in 5.7% (Table 3).
Table 3. Distribution of patients with extremely high lipoprotein (a) by the degree of brachiocephalic artery stenosis across age groups (n = 731)
|
BCA stenosis |
Age group |
p-value |
||||
|
18–24 (n = 2) |
25–44 (n = 175) |
45–59 (n = 295) |
60–74 (n = 205) |
≥75 (n = 54) |
||
|
<20% |
2 (100) |
49 (28.0) |
26 (8.8) |
8 (3.9) |
0 (0) |
<0.001 |
|
20–25% |
0 (0) |
91 (52.0) |
160 (54.2) |
63 (30.7) |
11 (20.4) |
|
|
26–34% |
0 (0) |
26 (14.9) |
72 (24.4) |
63 (30.7) |
11 (20.4) |
|
|
35–49% |
0 (0) |
5 (2.9) |
26 (8.8) |
33 (16.1) |
10 (18.5) |
|
|
50–55% |
0 (0) |
0 (0) |
5 (1.7) |
16 (7.8) |
12 (22.2) |
|
|
>55% |
0 (0) |
4 (2.3) |
6 (2.0) |
22 (10.7) |
10 (18.5) |
|
Notes: data are presented as the absolute number of patients with the characteristic and the proportion within the group, expressed as a percentage (in parentheses). Pearson χ² test was used for comparisons.
BCA – brachiocephalic arteries.
Already in the 25–44 age group, atherosclerotic involvement of the BCA (stenosis ≥ 20%) was present in the majority of evaluated patients (72.0%). In the 45–59 age group the prevalence of stenosis rose to 91.2%, in patients aged 60–74 years it reached 96.1%, and among patients aged ≥75 years atherosclerotic involvement of the BCA was detected in 100% of those evaluated (Table 3).
In the 25–59 age groups, mild and moderate forms of atherosclerosis (predominantly BCA stenoses of up to 35%) predominated, whereas more advanced lesions were relatively uncommon. With increasing age, the distribution shifted progressively toward more severe stenoses. The proportion of stenoses of ≥35% rose substantially in the 60–74 age group, and patients aged ≥ 75 years showed an accumulation of hemodynamically significant stenoses (>55%) together with a reduction in minimal lesions (p < 0.001).
Duplex ultrasound of the LEA was available for 36.8% (n = 407) of patients. In the 25–44 age group, atherosclerotic involvement of the LEA (stenosis ≥ 20%) was present in 74.8% of those evaluated. In the 45–59 age group the prevalence of LEA stenosis was 87.2%, in patients aged 60–74 years it reached 96.5%, and among patients aged ≥ 75 years atherosclerotic changes were detected in 100% of those evaluated (Table 4).
Table 4. Distribution of patients with extremely high lipoprotein (a) by the degree of lower extremity artery stenosis across age groups (n = 407)
|
LEA stenosis |
Age group |
p-value |
||||
|
18–24 (n = 1) |
25–44 (n = 103) |
45–59 (n = 156) |
60–74 (n = 114) |
≥75 (n = 33) |
||
|
<20% |
1 (100) |
26 (25.2) |
20 (12.8) |
4 (3.5) |
0 (0) |
<0.001 |
|
20–25% |
0 (0) |
54 (52.4) |
88 (56.4) |
48 (42.1) |
7 (21.2) |
|
|
26–34% |
0 (0) |
20 (19.4) |
35 (22.4) |
29 (25.4) |
6 (18.2) |
|
|
35–49% |
0 (0) |
3 (2.9) |
8 (5.1) |
13 (11.4) |
8 (24.2) |
|
|
50–55% |
0 (0) |
0 (0) |
0 (0) |
10 (8.8) |
4 (12.1) |
|
|
>55% |
0 (0) |
0 (0) |
5 (3.2) |
10 (8.8) |
8 (24.2) |
|
Notes: data are presented as the absolute number of patients with the characteristic and the proportion within the group, expressed as a percentage (in parentheses). Pearson χ² test was used for comparisons.
LEA – lower extremity arteries.
The age-related progression of atherosclerotic LEA involvement mirrored that observed in the BCA, with mild and moderate stenoses predominating in the 25–59 age groups and a rising proportion of hemodynamically significant stenoses in patients aged ≥ 60 years.
CACS was assessed in 11.9% (n = 132) of patients. Coronary calcification (CACS > 0) was detected in 50.0% (n = 66) of those examined, with its prevalence increasing with age. In the 25–44 age group, CACS > 0 was identified in 19.4% of patients; in the 45–59 age group, in 39.5%; in patients aged 60–74 years, in 59.1%; and among those aged ≥75 years, coronary calcification was present in 100% of those evaluated (Table 5).
Table 5. Distribution of patients with extremely high lipoprotein (a) by coronary artery calcium score across age groups (n = 132)
|
CACS |
Age group |
p-value |
|||
|
25–44 (n = 36) |
45–59 (n = 43) |
60–74 (n = 44) |
≥75 (n = 9) |
||
|
0 units |
27 (75.0) |
24 (55.8) |
15 (34.1) |
0 (0) |
<0.001 |
|
1–10 units |
4 (11.1) |
7 (16.3) |
7 (15.9) |
0 (0) |
|
|
11–100 units |
2 (5.6) |
8 (18.6) |
8 (18.2) |
4 (44.4) |
|
|
101–399 units |
3 (8.3) |
3 (7.0) |
8 (18.2) |
4 (44.4) |
|
|
≥400 units |
0 (0) |
1 (2.3) |
6 (13.6) |
1 (11.1) |
|
Notes: data are presented as the absolute number of patients with the characteristic and the proportion within the group, expressed as a percentage (in parentheses). Pearson χ² test was used for comparisons.
CACS – coronary artery calcium score.
In the 25–44 age group, only isolated cases of moderate or severe coronary calcification were observed. In the 45–59 age group, the proportion of patients with CACS values of 11–100 and 101–399 rose substantially, and in older age groups the distribution shifted markedly toward an increased frequency of severe and very severe coronary calcification.
Data on the assessment of all three vascular beds were available in 6.2% of patients (n = 68) from the age groups 25 years and older. Analysis of this subgroup showed that no signs of atherosclerosis were detected in only 2.9% (n = 2) of patients. Single-bed involvement was observed in 7.4% (n = 5) and two-bed involvement in 36.8% (n = 25), whereas more than half of the patients (52.9%, n = 36) had atherosclerotic involvement of all three evaluated vascular beds. The distribution of patients by the number of affected vascular beds across age groups is shown in Figure 3.
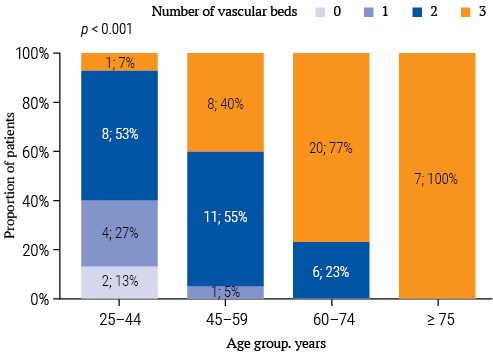
FIG. 3. Distribution of patients with extremely high lipoprotein (a) by the number of affected vascular beds (n = 68).
Combined involvement of multiple vascular beds showed a clear age-dependent pattern. In the 25–44 age group, the majority of patients evaluated (60.0%) had two- or three-bed involvement, and only 13.3% had no affected beds. In the 45–59 and 60–74 age groups, the proportion of patients with three-bed involvement increased progressively (40.0% and 76.9%, respectively), and by the age of ≥75 years, combined involvement of all three vascular beds was observed in 100% of patients (p < 0.001).
Among the 731 patients for whom vascular bed imaging data were available, 65.0% (n = 475) had no history of ASCVD, whereas 35.0% (n = 256) had documented ASCVD.
Among patients without ASCVD, atherosclerotic involvement of the BCA was detected in 85.9% of cases (408 of 475 patients evaluated), LEA involvement in 82.6% (209 of 253), and coronary calcification in 37.1% (33 of 89).
By comparison, the frequency of imaging-detected vascular involvement was predictably higher among patients with documented ASCVD: BCA stenosis – 98.1%, LEA stenosis – 98.1%, and coronary calcification – 76.7% (p < 0.001 for all comparisons) (Fig. 4).
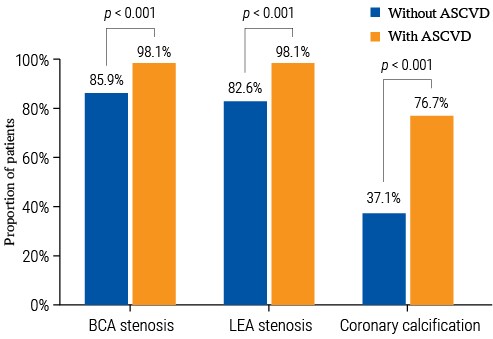
FIG. 4. Frequency of atherosclerotic vascular bed involvement in patients with and without documented atherosclerotic cardiovascular disease.
Notes: Pearson χ² test was used for comparisons.
ASCVD – atherosclerotic cardiovascular disease; BCA – brachiocephalic arteries; LEA – lower extremity arteries.
The present study characterizes one of the least well-described categories of patients in routine clinical practice – individuals with extremely high Lp(a) (≥180 mg/dL).
The study cohort comprised 1105 patients, accounting for 1.09% of the source database, which is consistent with international population estimates: in a large US registry of more than 500,000 individuals, an Lp(a) level of ≥180 mg/dL corresponded to the 99th percentile of the distribution [12]. In an Israeli study of approximately 4000 patients, the prevalence of extremely high Lp(a) was 1.3% [13].
Notably, 29.5% of patients in our cohort had a history of ASCVD. By comparison, in the ESSE-RF study the prevalence of CAD among Russian adults aged 25–64 years was 5.7% [14], and the general population prevalence of CAD in the Russian Federation did not exceed 13.5% [15]. Thus, the frequency of ASCVD in the study cohort substantially exceeds population estimates, indirectly supporting an independent contribution of extremely high Lp(a) to an unfavorable cardiovascular prognosis.
At the national level, data from ESSE-RF show a pronounced right-skewed distribution of Lp(a) and a substantial proportion of individuals with elevated values, with an increase in ASCVD risk already apparent at Lp(a) > 9 mg/dL [6]. Within this context, the Lp(a) ≥ 180 mg/dL group represents the most extreme segment of the population, with a very high lifetime risk. The clinical importance of this range is underscored by Russian registry data: in the REGION-MI study, Lp(a) > 180 mg/dL was detected in approximately 1 in 10 patients with myocardial infarction [16]. This emphasizes that extreme Lp(a) values are not a rarity but a practical concern for timely prevention and onward referral.
The lipid profile in our cohort was characterized by a combination of severe hypercholesterolemia and age-related changes in atherogenic lipid fractions. This phenotype is consistent with Russian population observations, in which Lp(a) showed positive associations with TC, LDL-C, and the apoB/apoA-I ratio [17]. This in part implies the presence of a modifiable risk layer (LDL-C/apoB) overlying the non-modifiable Lp(a) component, making this population potentially manageable when treatment is intensified in a timely manner.
Interpretation of LDL-C in individuals with very high Lp(a) requires caution: a portion of measured or calculated LDL-C may reflect cholesterol carried by Lp(a) particles, while approaches to correcting LDL-C for Lp(a)-cholesterol are not yet standardized [2]. In practical terms, this means that even with only moderately elevated LDL-C, a patient with Lp(a) ≥ 180 mg/dL may retain a very high lifetime risk and may require more aggressive correction of risk factors than predicted by traditional risk scores.
It is worth noting that in real-world practice, even in patients with extremely high Lp(a), lipid-lowering therapy is often suboptimally intensified, and LDL-C targets are achieved in only a fraction of patients.
In the cross-sectional study by B. Zafrir et al. [13], only 33% of patients with Lp(a) > 430 nmol/L and CAD were receiving combination therapy with a statin and ezetimibe, and only 36% of those achieved an LDL-C target of < 55 mg/dL. At the same time, the prevalence of myocardial infarction (47.2% vs. 18.9%), CAD (62.3% vs. 28.3%), and peripheral artery disease and stroke (22.6% vs. 11.3%) was substantially higher in patients with Lp(a) > 430 nmol/L compared with those with values < 72 nmol/L [13].
Against this background, patients with extremely high Lp(a) represent a priority population both for classical LDL-C-lowering interventions and for the prospective introduction of Lp(a)-targeted therapy, which has demonstrated pronounced reductions in Lp(a) in early-phase clinical trials [18]. At present, the only available method of substantially lowering elevated Lp(a) levels is Lp(a) apheresis, used for secondary prevention when maximally tolerated lipid-lowering therapy proves insufficient [19].
Our data show relative age-related stability of Lp(a) within the extreme range, consistent with the concept of early detection – including a one-time, lifetime measurement – followed by risk-based referral and follow-up [4].
A high prevalence of multifocal atherosclerosis was observed in the study cohort. This finding is consistent with data from the largest contemporary population-based analysis from China by S. Man et al. [20], which included approximately 2.9 million adults and showed that elevated Lp(a) was associated with subclinical atherosclerosis, with the effect being more pronounced for severe and multi-site involvement; the authors explicitly emphasize the need for comprehensive assessment of subclinical atherosclerosis in individuals with elevated Lp(a).
It should be emphasized that, in our study, full assessment of all three vascular beds was performed in only a limited number of patients, reflecting the systematic real-world under-evaluation of multifocal involvement. This in itself is an argument in favor of a standardized management algorithm for patients with extreme Lp(a) values, as an essential prerequisite for accurate risk re-stratification.
Our findings indicate an early onset, high prevalence and age-dependent nature of the atherosclerotic process in the study cohort. Additional support comes from the ESSE-RF sub-study ATEROGEN-Ivanovo [21], in which the prevalence of at least one atherosclerotic plaque in the carotid or femoral arteries among individuals aged 40–67 years was 73.6%, with plaques being detected as early as the age of 40 years. Comparable findings have been reported in the PESA study [22]: among more than 4000 asymptomatic individuals aged 40–54 years, subclinical atherosclerosis was identified in 63% of participants. Although Lp(a) was not assessed in those studies, they demonstrate a high prevalence of subclinical atherosclerosis in the working-age population and indirectly support the hypothesis of an earlier and more severe multifocal atherosclerotic phenotype in individuals with Lp(a) ≥ 180 mg/dL.
In our cohort, coronary artery calcium screening in patients with extremely high Lp(a) reveals a clear age-related gradient not only in the frequency but also in the severity of coronary atherosclerosis. This supports the clinical value of CACS as a tool for refining individual cardiovascular risk assessment in this patient population. Further support for this approach comes from a pooled analysis of a multi-ethnic cohort, in which Lp(a) and CACS showed independent and additive effects on ASCVD risk, with the combination of CACS > 100 units and the top Lp(a) quintile being associated with an almost 5-fold increase in risk [23]. Thus, the combined assessment of these two markers identifies the highest-risk subgroups and helps to refine strategic decisions in primary prevention.
These findings, consistent with international observations, support the need for a standardized approach to identifying patients with extremely high Lp(a), with subsequent implementation of preventive programs and a system of follow-up. In particular, the Brussels International Declaration on Lp(a) Testing and Management calls for the integration of Lp(a) screening and patient referral into national cardiovascular health strategies, including a one-time, lifetime measurement in every adult [24]. In the United States, systemic initiatives are being implemented to improve detection of high-risk groups – for example, the FIND-Lp(a) project, which is developing a machine-learning model to analyze electronic medical records, identify individuals with a high likelihood of elevated Lp(a), and refer them for confirmatory laboratory testing3.
Our study is a single-center retrospective analysis, which limits the generalizability of the findings and precludes strict causal inferences. In addition, only patients with extremely high Lp(a) were included, and a complete assessment of all three vascular beds was performed only in a subset of patients, which may lead to an underestimation of the prevalence of multifocal atherosclerosis and complicate the extrapolation of these findings to patients with less marked Lp(a) elevations.
Promising directions for future research include large prospective studies with long-term follow-up of clinical outcomes in patients with extremely high Lp(a) and multifocal subclinical atherosclerosis, as well as the comparison of different screening and risk re-stratification algorithms incorporating Lp(a), CACS and vascular imaging. In addition, interventional trials of Lp(a)-targeted therapy with assessment of effects on subclinical atherosclerosis and cardiovascular events are warranted, as are efforts to standardize Lp(a) measurement and refine risk thresholds.
Patients with extremely high Lp(a) (≥180 mg/dL) constitute a phenotype with very high lifetime cardiovascular risk and are characterized by early development of subclinical atherosclerosis. Even in young adulthood, the majority of these patients show signs of multifocal atherosclerosis, highlighting the limitations of traditional risk stratification approaches, which rely primarily on age and classical risk factors. These findings support the use of an Lp(a) threshold of ≥180 mg/dL as a simple and reproducible criterion for identifying a priority group warranting in-depth multi-bed vascular assessment, early risk re-stratification, and more intensive correction of modifiable risk factors, as well as a promising platform for the development of systemic atherosclerotic cardiovascular disease prevention.
Mikhail G. Chashchin developed the research idea and study design, participated in concept discussion, data analysis and verification, interpretation of results, critical revision, and manuscript writing. Zalina I. Khutaeva developed the study protocol, performed cohort selection and data verification, and participated in data analysis and interpretation, manuscript writing, and article editing. Maxim B. Mukhtarov extracted data from electronic medical records, developed the database, and participated in statistical analysis, preparation of graphical materials, and article editing. Zubaidat M. Musaeva and Khava A. Khashieva performed clinical data verification and participated in the interpretation of results and article editing. Vadim L. Averkiev reviewed clinical data and exclusion criteria and participated in the interpretation of results and article editing. Venera S. Rabicheva collected and processed the data and participated in the interpretation of results and article editing. Gennady A. Konovalov and Alexander Yu. Gorshkov participated in discussion of the study concept and methodology, critical revision of the manuscript, and article editing. Gennady A. Konovalov also participated in the interpretation of results. Oksana M. Drapkina provided overall scientific supervision and critically revised the manuscript for important intellectual content. All authors approved the final version of the article.
Compliance with ethical standards. The study was conducted in accordance with the principles of the Declaration of Helsinki. The retrospective design using anonymized data did not require additional approval from the local ethics committee. At the initial visit, all patients signed informed consent for the processing of personal data.
Data availability. The data confirming the findings of this study are available from the authors upon reasonable request. Data and statistical methods used in the article were examined by a professional biostatistician on the Sechenov Medical Journal editorial staff.
Conflict of interest. The authors declare that there is no conflict of interests.
Financing. The study was not sponsored (own resources).
Use of artificial intelligence. No artificial intelligence tools were used in the preparation of this manuscript.
1. Decree of the Government of the Russian Federation No. 2188 of 29 December 2025 “On the Program of State Guarantees of Free Provision of Medical Care for 2026 and the planning period of 2027 and 2028”. https://dgp69.mos.ru/public/docs/legaldoc/pprf-29-12-2025-2188.pdf (access date: 09.02.2026).
2. MedStat.Pro: web application for statistical analysis of medical data [computer software]. Version 0.8.1. Russian software registration certificate No. 2025688091 dated 16 October 2025. Moscow; 2026. https://app.medstat.pro (access date: 15.02.2026).
3. The Family Heart Foundation. FIND Lp(a). https://familyheart.org/find/find-lpa (access date: 09.02.2026).
1. Afanasyeva O.I., Pokrovsky S.N. Lipoprotein (a) as underestimated cardiovascular risk factor in Russia. Time to introduce into clinical practice. Russian Journal of Cardiology. 2024; 29(8): 6035. (In Russian). https://doi.org/10.15829/1560-4071-2024-6035. EDN: ABZKLD
2. Koschinsky M.L., Bajaj A., Boffa M.B., et al. A focused update to the 2019 NLA scientific statement on use of lipoprotein (a) in clinical practice. J Clin Lipidol. 2024 May-Jun; 18(3): e308–e319. https://doi.org/10.1016/j.jacl.2024.03.001. Epub 2024 Apr 1. PMID: 38565461
3. Ezhov M.V., Kukharchuk V.V., Balakhonova T.V., et al. Eurasian Association of Cardiology / Russian National Atherosclerosis Society Guidelines for the diagnosis and correction of dyslipidemia for the prevention and treatment of atherosclerosis (2025). Eurasian Heart Journal. 2025; 26(1): 6–34 (In Russian). https://doi.org/10.38109/2225-1685-2025-2-6-34. EDN: MACELC
4. Voevoda M.I., Ezhov M.V., Konovalov G.A., et al. New opportunities to use a lipoprotein (a) blood test in real-life clinical practice. Resolution of the expert council. Russian Medical Journal. 2024; 9(2): 40–44 (In Russian). https://doi.org/10.32364/2225-2282-2024-9-7. EDN: WFHYUT
5. Kronenberg F., Mora S., Stroes E.S.G., et al. Lipoprotein (a) in atherosclerotic cardiovascular disease and aortic stenosis: a European Atherosclerosis Society consensus statement. Eur Heart J. 2022 Oct; 43(39): 3925–3946. https://doi.org/10.1093/eur-heartj/ehac361. PMID: 36036785
6. Ezhov M.V., Shalnova S.A., Yarovaya E.B., et al. Lipoprotein (a) in an adult sample from the Russian population: distribution and association with atherosclerotic cardiovascular diseases. Arch Med Sci. 2021 Mar; 19(4): 995–1002. https://doi.org/10.5114/aoms/131089. PMID: 37560742
7. Khutaeva Z.I., Konovalov G.A. Lipoprotein (a): new approaches in risk assessment and management. Atherosclerosis and Dyslipidemias. 2025; 1(58): 5–12 (In Russian). https://doi.org/10.34687/2219-8202. JAD.2025.01.0001. EDN: SWYSZT
8. Kamstrup P.R., Benn M., Tybjærg-Hansen A., Nordestgaard B.G. Extreme lipoprotein (a) levels and risk of myocardial infarction in the general population. Circulation. 2008 Jan; 117(2): 176–184. https://doi.org/10.1161/CIRCULATIONAHA.107.715698. Epub 2007 Dec 17. PMID: 18086931
9. Thomas P.E., Vedel-Krogh S., Nielsen S.F., et al. Lipoprotein (a) and risks of peripheral artery disease, abdominal aortic aneurysm, and major adverse limb events. J Am Coll Cardiol. 2023 Dec; 82(24): 2265–2276. https://doi.org/10.1016/j.jacc.2023.10.009. PMID: 38057068
10. Kamstrup P.R., Tybjærg-Hansen A., Nordestgaard B.G. Elevated lipoprotein (a) and risk of aortic valve stenosis in the general population. J Am Coll Cardiol. 2014 Feb; 63(5): 470–477. https://doi.org/10.1016/j.jacc.2013.09.038. Epub 2013 Oct 23. PMID: 24161338
11. Nordestgaard A.T., Chasman D.I., Moorthy V., et al. Thirty-year risk of cardiovascular disease among healthy women according to clinical thresholds of lipoprotein (a). JAMA Cardiol. 2026 Feb; 11(2): 175–185. https://doi.org/10.1001/jamacardio.2025.5043. PMID: 41499112
12. Varvel S., McConnell J.P., Tsimikas S. Prevalence of elevated Lp(a) mass levels and patient thresholds in 532 359 patients in the United States. Arterioscler Thromb Vasc Biol. 2016 Nov; 36(11): 2239–2245. https://doi.org/10.1161/atvbaha.116.308011. Epub 2016 Sep 22. PMID: 27659098
13. Zafrir B., Aker A., Saliba W. Extreme lipoprotein (a) in clinical practice: a cross sectional study. Int J Cardiol Cardiovasc Risk Prev. 2023 Jan; 16: 200173. https://doi.org/10.1016/j.ijcrp.2023.200173. PMID: 36874038
14. Muromtseva G.A., Vilkov V.G., Konstantinov V.V., et al. The prevalence of electrocardiographic abnormalities in the Russian population in the early 21st century (the ESSE-RF study). Russian Journal of Cardiology. 2018; 23(12): 7–17 (In Russian). https://doi.org/10.15829/1560-4071-2018-12-7-17. EDN: YPPAWL
15. Shalnova S.A., Deev A.D. Coronary heart disease in Russia: incidence rate and treatment according to epidemiological data. Therapeutic Archive. 2011; 83(1): 7–12 (In Russian)
16. Ezhov M.V., Shakhnovich R.M., Alekseeva I.A., et al. Prevalence and role of elevated serum lipoprotein (a) in patients with myocardial infarction according to the Russian register of acute myocardial infarction REGIONMI. Cardiological Bulletin. 2025; 20(1): 39–48 (In Russian). https://doi.org/10.17116/Cardiobulletin20252001139 . EDN: WADXRV
17. Shalnova S.A., Ezhov M.V., Metelskaya V.A., et al. Association between lipoprotein (a) and risk factors of atherosclerosis in Russian population (data of observational ESSE-RF study). Rational Pharmacotherapy in Cardiology. 2019; 15(5): 612–621 (In Russian). https://doi. org/10.20996/1819-6446-2019-15-5-612-621. EDN: KBMFPI
18. O’Donoghue M.L., Rosenson R.S., Gencer B., et al. Small interfering RNA to reduce lipoprotein (a) in cardiovascular disease. N Engl J Med. 2022 Nov; 387(20): 1855–1864. https://doi.org/10.1056/NEJMoa2211023. Epub 2022 Nov 6. PMID: 36342163
19. Pokrovsky S.N., Afanasieva O.I., Safarova M.S., et al. Specific Lp(a) apheresis: A tool to prove lipoprotein (a) atherogenicity. Atheroscler Suppl. 2017 Nov; 30: 166–173. https://doi.org/10.1016/j.atherosclerosissup.2017.05.004. Epub 2017 May 31. PMID: 29096833
20. Man S., Zu Y., Yang X., et al. Prevalence of elevated lipoprotein (a) and its association with subclinical atherosclerosis in 2.9 million Chinese adults. J Am Coll Cardiol. 2025 Jun; 85(21): 1979–1992. https://doi.org/10.1016/j.jacc.2025.02.032. Epub 2025 Apr 23. PMID: 40266173
21. Ershova A.I., Balakhonova T.V., Meshkov A.N., et al. Prevalence of carotid and femoral artery atherosclerosis among the Ivanovo Oblast population: data from the ATEROGEN-Ivanovo study. Cardiovascular Therapy and Prevention. 2021; 20(5): 2994 (In Russian). https://doi.org/10.15829/1728-8800-2021-2994. EDN: BFATEF
22. Fernández-Friera L., Peñalvo J.L., Fernández-Ortiz A., et al. Prevalence, vascular distribution, and multiterritorial extent of subclinical atherosclerosis in a middle-aged cohort. Circulation. 2015 Jun; 131(24): 2104–2113. https://doi.org/10.1161/CIRCULATIONAHA.114.014310. Epub 2015 Apr 16. PMID: 25882487
23. Mehta A., Vasquez N., Ayers C.R., et al. Independent association of lipoprotein (a) and coronary artery calcification with atherosclerotic cardiovascular risk. J Am Coll Cardiol. 2022 Mar; 79(8): 757–768. https://doi.org/10.1016/j.jacc.2021.11.058. PMID: 35210030
24. Kronenberg F., Bedlington N., Ademi Z., et al. The Brussels International declaration on lipoprotein (a) testing and management. Atherosclerosis. 2025; 406: 119218. https://doi.org/10.1016/j.atherosclerosis.2025.119218. Epub 2025 May 5. PMID: 40340180
Mikhail G. Chashchin, Cand. of Sci. (Medicine), cardiologist, lipidologist, Head of the Lipid Clinic.
10/3, Petroverigsky Ln., Moscow, 101990
Zalina I. Khutaeva - postgraduate student, National Medical Research Center for Therapy and Preventive Medicine; сardiologist, lipidologist, MEDSI CDC at Belorusskaya.
10/3, Petroverigsky Ln., Moscow, 101990; 3A, Gruzinsky Ln., Moscow, 123056
Gennady A. Konovalov - Dr. of Sci. (Medicine), Professor, Head of the Center for Diagnostics and Innovative Medical Technologies, MEDSI CDC at Belorusskaya.
3A, Gruzinsky Ln., Moscow, 123056
Maxim B. Mukhtarov - Director of the Data Management Department, MEDSI Digital LLC.
5, Uspenskaya str., Krasnogorsk, 143409
Zubaidat M. Musaeva - сardiologist, Head of the Cardiology Department, MEDSI CDC at Belorusskaya.
3A, Gruzinsky Ln., Moscow, 123056
Khava A. Khashieva - cardiologist, lipidologist, MEDSI CDC at Belorusskaya.
3A, Gruzinsky Ln., Moscow, 123056
Vadim L. Averkiev - Cand. of Sci. (Medicine), transfusiologist, Head of the Department of Extracorporeal Methods of Treatment, Center for Diagnostics and Innovative Medical Technologies, MEDSI CDC at Belorusskaya.
3A, Gruzinsky Ln., Moscow, 123056
Venera S. Rabicheva - transfusiologist, Department of Extracorporeal Methods of Treatment, Center for Diagnostics and Innovative Medical Technologies, MEDSI CDC at Belorusskaya.
3A, Gruzinsky Ln., Moscow, 123056
Alexander Yu. Gorshkov - Cand. of Sci. (Medicine), Deputy Director for Research and Outpatient Clinical Activities, National Medical Research Center for Therapy and Preventive Medicine.
10/3, Petroverigsky Ln., Moscow, 101990
Oksana M. Drapkina - Dr. of Sci. (Medicine), Professor, Academician of the RAS, Director of the National Medical Research Center for Therapy and Preventive Medicine; Chief External Expert in Internal Medicine and General Practice of the Ministry of Health of the Russian Federation.
10/3, Petroverigsky Ln., Moscow, 101990

|
1. Дополнительные материалы | |
| Subject | ||
| Type | Исследовательские инструменты | |
Download
(899KB)
|
Indexing metadata ▾ | |
|
|
2. Supplementary materials | |
| Subject | ||
| Type | Исследовательские инструменты | |
Download
(1MB)
|
Indexing metadata ▾ | |
|
|
3. STROBE checklist | |
| Subject | ||
| Type | Исследовательские инструменты | |
Download
(207KB)
|
Indexing metadata ▾ | |
Sechenov Medical Journal. Editor's checklist for this article you can find here.
Название / Title | Экстремально высокий липопротеин (а) как маркер раннего атеросклероза: анализ крупной когорты реальной практики / Extremely high lipoprotein (a) as a marker of early atherosclerosis: analysis of a large real-world cohort
|
Раздел / Section
| ВНУТРЕННИЕ БОЛЕЗНИ/ INTERNAL MEDICINE
|
Тип / Article | Оригинальная статья / Original article |
Номер / Number | 1492
|
Страна/территория / Country/Territory of origin | Россия / Russia |
Язык / Language | Русский / Russian Английский / English
|
Источник / Manuscript source | Инициативная рукопись / Unsolicited manuscript |
Дата поступления / Received | 28.01.2026 |
Тип рецензирования / Type ofpeer-review | Двойное слепое / Double blind |
Язык рецензирования / Peer-review language | Русский / Russian
|
РЕЦЕНЗЕНТ А / REVIEWER A
Инициалы / Initials | 1492_А
|
Научная степень / Scientific degree | Доктор медицинских наук / Dr. of Sci. (Medicine)
|
Страна/территория / Country/Territory | Россия / Russia
|
Дата рецензирования / Date of peer-review | 26.02.2026 |
Число раундов рецензирования / Number of peer-review rounds | 1 |
Финальное решение / Final decision | принять к публикации / accept
|
ПЕРВЫЙ РАУНД РЕЦЕНЗИРОВАНИЯ / FIRST ROUND OF PEER-REVIEW
Современное оригинальное исследование по взаимосвязи поражения сосудов атеросклерозом и уровня Лп(а). Хорошо проиллюстрировано. Выборка достаточная. Статистические методы адекватные.
ЗАКЛЮЧЕНИЕ: принять к публикации.
РЕЦЕНЗЕНТ B / REVIEWER B
Инициалы / Initials | 1492_В
|
Научная степень / Scientific degree | Кандидат медицинских наук / Cand. of Sci. (Medicine)
|
Страна/территория / Country/Territory | Россия / Russian
|
Дата рецензирования / Date of peer-review | 11.03.2026 |
Число раундов рецензирования / Number of peer-review rounds | 1 |
Финальное решение / Final decision | принять к публикации после небольшой доработки/ minor revision
|
ПЕРВЫЙ РАУНД РЕЦЕНЗИРОВАНИЯ / FIRST ROUND OF PEER-REVIEW
В настоящее время выбранная тематика статьи является важным направлением в кардиологии, особенно учитывая распространенность и смертность от сердечно-сосудистых заболеваний в РФ.
Представлены актуальные данные о распространенности субклинического атеросклероза среди пациентов с уровнем Лп(а) ≥ 180 мг/дл.
Замечания и рекомендации рецензента:
ЗАКЛЮЧЕНИЕ: принять к публикации после небольшой доработки.
РЕКОМЕНДАЦИИ НАУЧНЫХ РЕДАКТОРОВ ЖУРНАЛА / RECOMMENDATIONS
OF THE SCIENTIFIC EDITORS OF THE JOURNAL
Рукопись посвящена актуальной клинической проблеме: значению экстремально высокого уровня липопротеина(а) как маркера раннего и мультифокального атеросклероза у пациентов реальной клинической практики. Исследование основано на крупной выборке из 1105 пациентов, отобранных из базы 101 078 амбулаторных наблюдений, и демонстрирует клинически значимые данные о высокой распространенности субклинического поражения БЦА, АНК и коронарного кальциноза уже в молодом возрасте. Работа обладает несомненной научной и практической значимостью, соответствует профилю журнала
Авторами последовательно изложены цель исследования, дизайн, основные характеристики когорты и ключевые результаты, касающиеся возрастной динамики атеросклеротического поражения различных сосудистых бассейнов. Особенно ценным является акцент на молодых возрастных группах и попытка обосновать необходимость выделения пациентов с Лп(а) ≥180 мг/дл в отдельный профилактический контур.
Вместе с тем рукопись нуждается в доработке:
ЗАКЛЮЧЕНИЕ: принять к публикации после небольшой доработки.

8-2 Trubetskaya st., Moscow, 119048
Federal State Autonomous Educational Institution of Нigher Education I.M.Sechenov First Moscow State Medical University of the Ministry of Health of the Russian Federation (Sechenovskiy University)
E-mail: sechenovmedj@staff.sechenov.ru
Processing of personal data
































