


ОBSTETRICS AND GYNECOLOGY
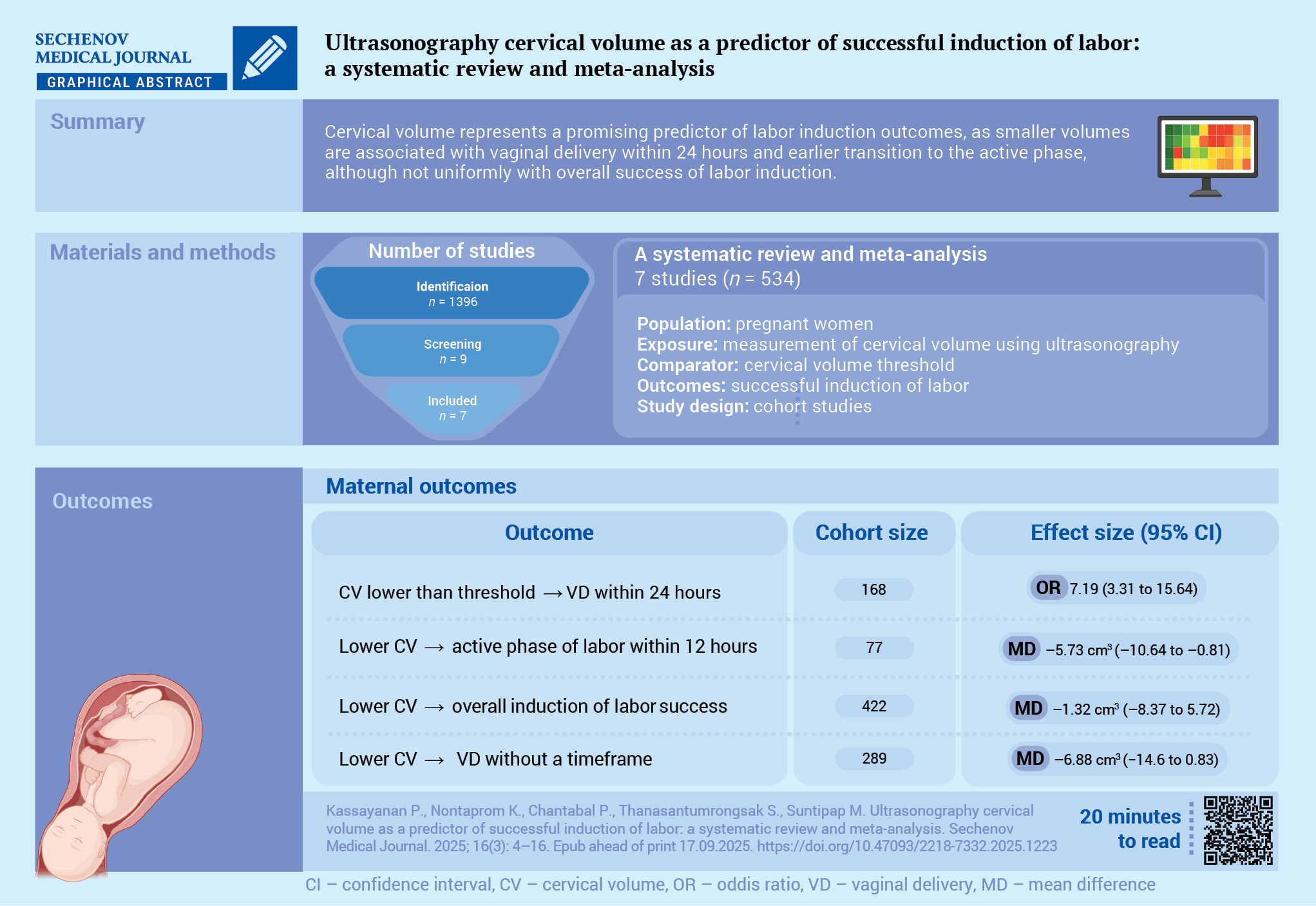
Aim. To compare the cervical volume of patients who underwent successful and failed induction of labor (IOL) procedures.
Materials and methods. This systematic review and meta-analysis were conducted according to PRISMA guidelines. A comprehensive literature search was performed in PubMed, EMBASE, Scopus, and Google Scholar to identify cohort studies published between January 01, 2005 and December 31, 2024, that compared cervical volume in pregnant women who underwent IOL. A random-effects meta-analysis was performed.
Results. Seven studies involving 534 pregnant women were included. Four studies were considered low risk of bias and two studies were regarded as high risk of bias. Risk of bias assessment could not be performed in one study because the full-text of the article was not available. The pooled analysis of two studies involving 168 pregnant women demonstrated a positive association between the lower cervical volume and successful vaginal delivery within 24 hours (odds ratio 7.19; 95% confidence interval: 3.31 to 15.64; I² = 0%). The pooled analysis of five studies involving 422 pregnant women showed no statistically significant difference between successful and failed IOL, with a mean difference –1.32 cm3; 95% confidence interval: –8.37 to 5.72; I² = 89.8%). Subgroup analyses showed no statistically significant association between cervical volume and successful IOL when defined as vaginal delivery without time restriction or within 24 hours. However, a significantly lower cervical volume was observed in women who achieved the active phase of labor within 12 hours. The Egger’s regression test confirmed the absence of small‑study effects (coefficient = 0.50, standard error = 1.75, p = 0.78).
Conclusion. Cervical volume has significant potential as a parameter for predicting successful IOL, with a smaller cervical volume being associated with better outcomes, although subgroup findings remain inconsistent.
NEUROSURGERY
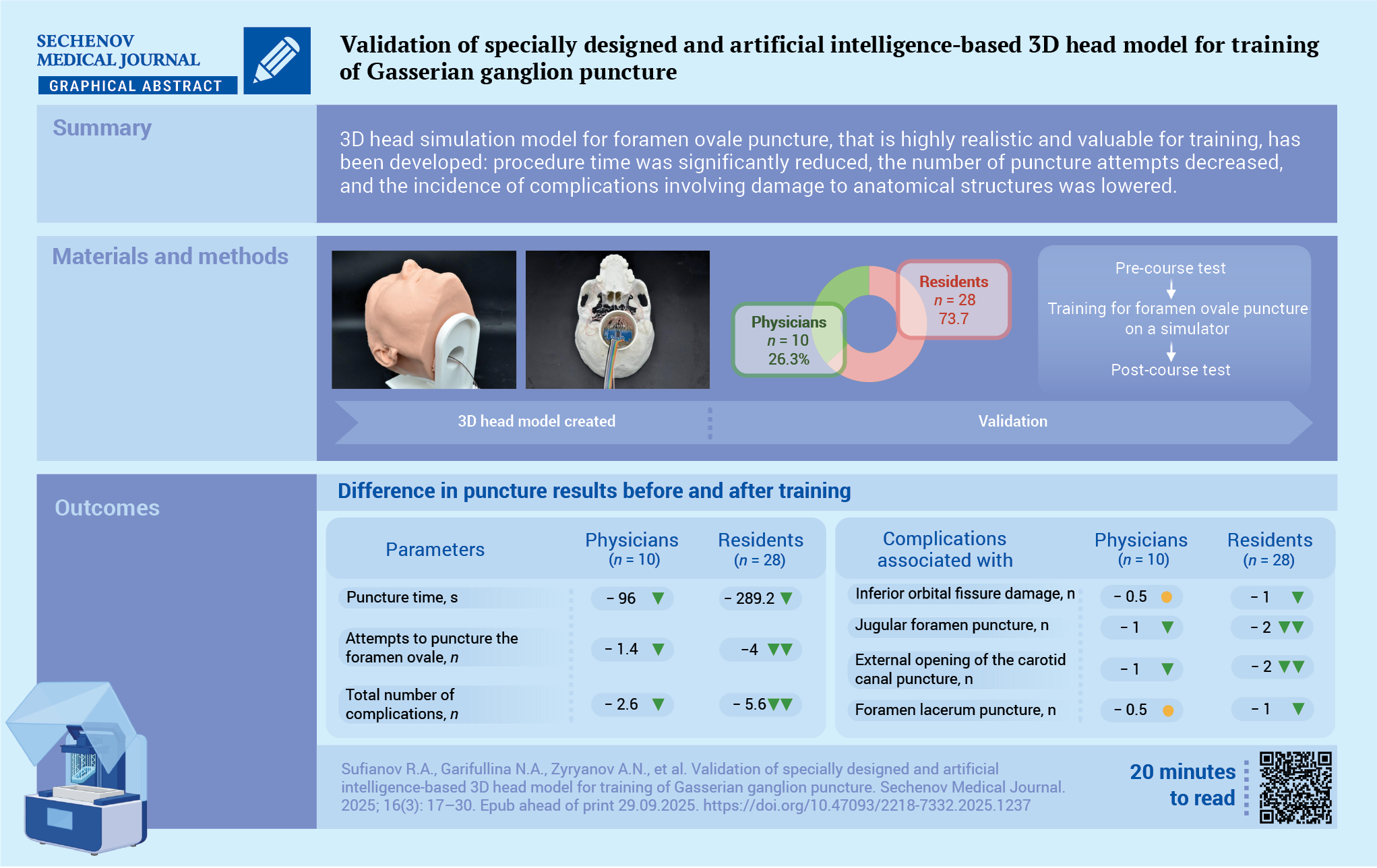
Aim. To design, develop and validate a 3D head simulation model for foramen ovale puncture, incorporating computer vision-based artificial intelligence (AI) technologies.
Materials and methods. A 3D simulation model with AI integration was developed in the prototyping laboratory. Its effectiveness for surgical training was evaluated by two groups: neurosurgeons with five or more years of experience (n = 10) and residents (n = 28). Training outcomes were assessed using the following parameters: intervention time, number of puncture attempts until they achieved the first one without any complications, number of complications involving critical anatomical structures. The validity was assessed using a Likert scale.
Results. Before the training session, the groups differed in terms of the time spent on the procedure, the number of puncture attempts and the number of complications involving critical anatomical structures. Post-training intervention time decreased by 50% in both groups, the number of puncture attempts reduced by 50.0% in physicians and by 60.3% in residents. The cumulative number of complications declined by 57.8% in physicians and by 59% in residents. Likert scale analysis revealed no statistically significant differences between groups across all parameters. The feasibility and educational effectiveness of the model were rated as 4 or 5 by 90% of participants in both groups. Anatomical realism received a score of 4 or 5 from 90% of physicians and 100% of residents. Radiographic realism received a score of 4 or 5 from all participants. The cost of creating a simulator, excluding the cost of a 3D printer, was 22,685 rubles.
Conclusion. The developed 3D simulation model with AI integration significantly improved training outcomes both in physicians’ and residents’ groups. The use of standard prototyping equipment provides a cost-effective, radiation-free alternative for widespread implementation in neurosurgical education.
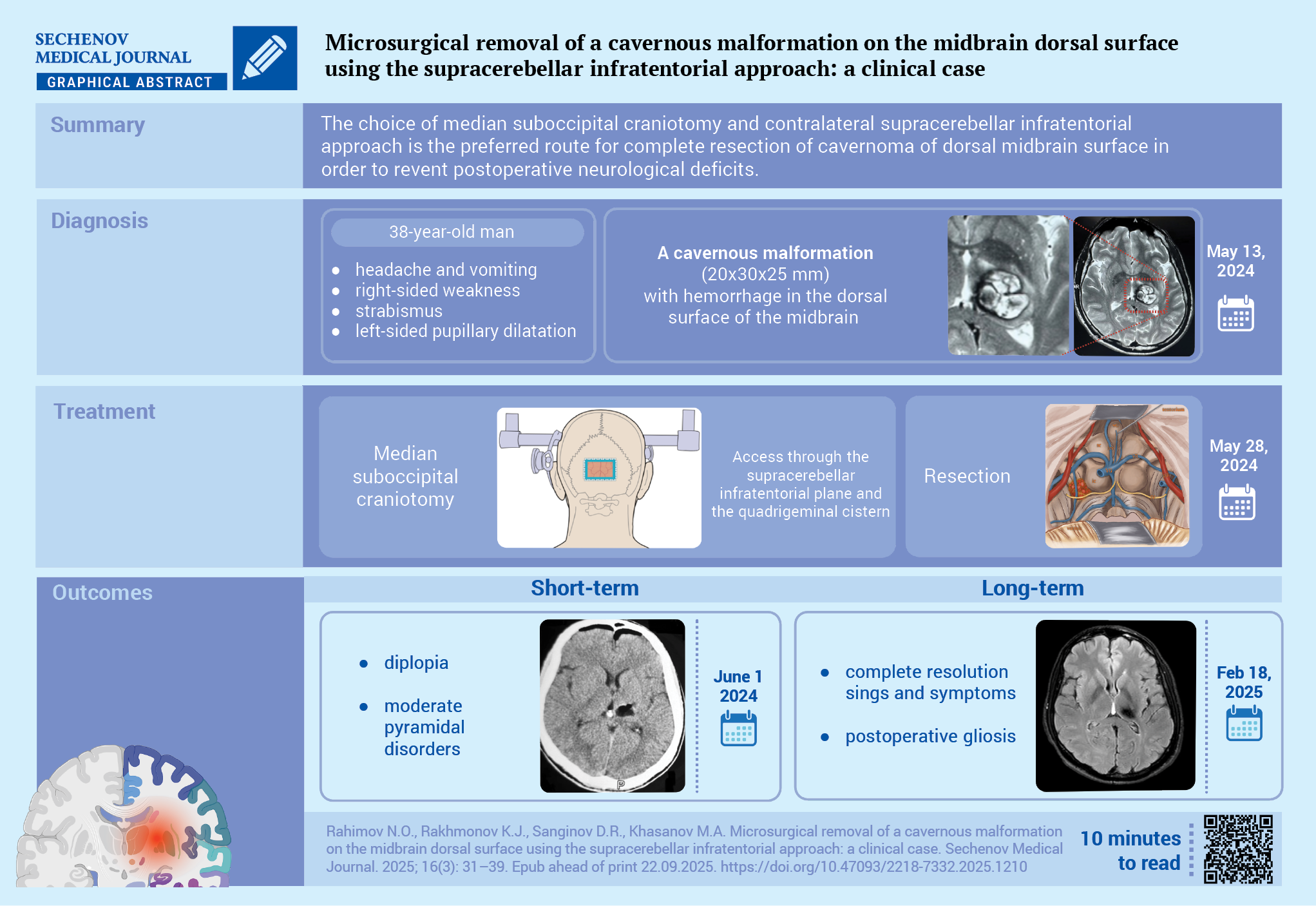
Common surgical approaches to the dorsal midbrain include: the occipital transtentorial, supracerebellar infratentorial, posterior subtemporal, and the tonsilloveal transaqueductal approaches.
Case report. A 38-year-old man presented with mild right-sided weakness and diplopia following an episode of headache and vomiting two weeks prior to admission. A neurological examination revealed mild right-sided weakness, a downward and outward strabismus, a mild left ocular mydriasis and accommodation paralysis alongside alternating syndrome. Magnetic resonance imaging revealed a 20×30×25 mm rupture of the cavernous malformation of the left midbrain peduncle as well as hematomas within the cavernoma. Using the supracerebellar infratentorial approach in a sitting position with minimal incision of dorsal midbrain, the cavernoma was completely resected together with surrounding subacute hematoma. In the early postoperative period, a regression of neurological symptoms was observed.
Discussion. The choice of median suboccipital craniotomy and contralateral supracerebellar infratentorial approach is the preferred route for complete resection of cavernoma of dorsal midbrain surface in order to avoid any postoperative neurological deficit.
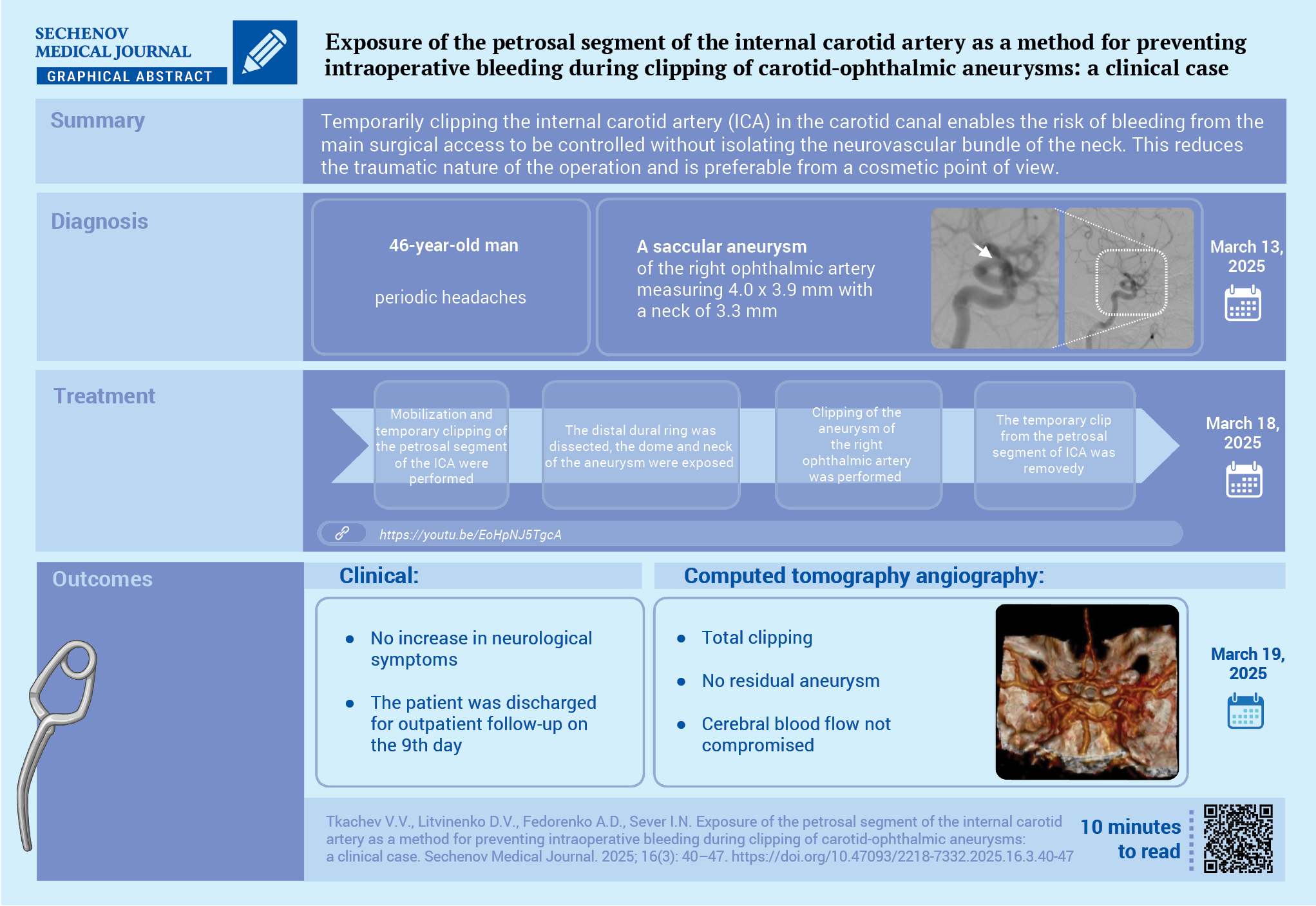
Microsurgical treatment of ocular artery aneurysms is classified as high-risk surgery. It is anatomically impossible to prevent and stop bleeding from ophthalmic aneurysms by applying a standard clip proximal to the aneurysm.
Case report. A 46-year-old man was admitted complaining of periodic headaches for 6 months. Outpatient magnetic resonance imaging revealed an aneurysm of the right internal carotid artery (ICA). According to computed tomography and cerebral angiography, an aneurysm of the ocular artery was verified. The patient chose an open surgery from the proposed treatment methods. Clipping of the aneurysm of the ocular artery mouth was performed by pterion access with an extradural extraction of the petrosal segment of the ICA to prevent intraoperative bleeding. The course of the postoperative period was smooth, without neurological symptoms, and the stitches were removed on the 9th day. The patient was discharged under outpatient supervision with a recommendation to control the radicality of clipping after 6 months.
Discussion. Temporary clipping of the ICA in the carotid canal during microsurgical operations for ocular artery aneurysms allows controlling the risk of bleeding from the main surgical access without isolating the neurovascular bundle of the neck, which reduces the traumatic nature of the operation and is preferable from a cosmetic point of view.
INTERNAL MEDICINE
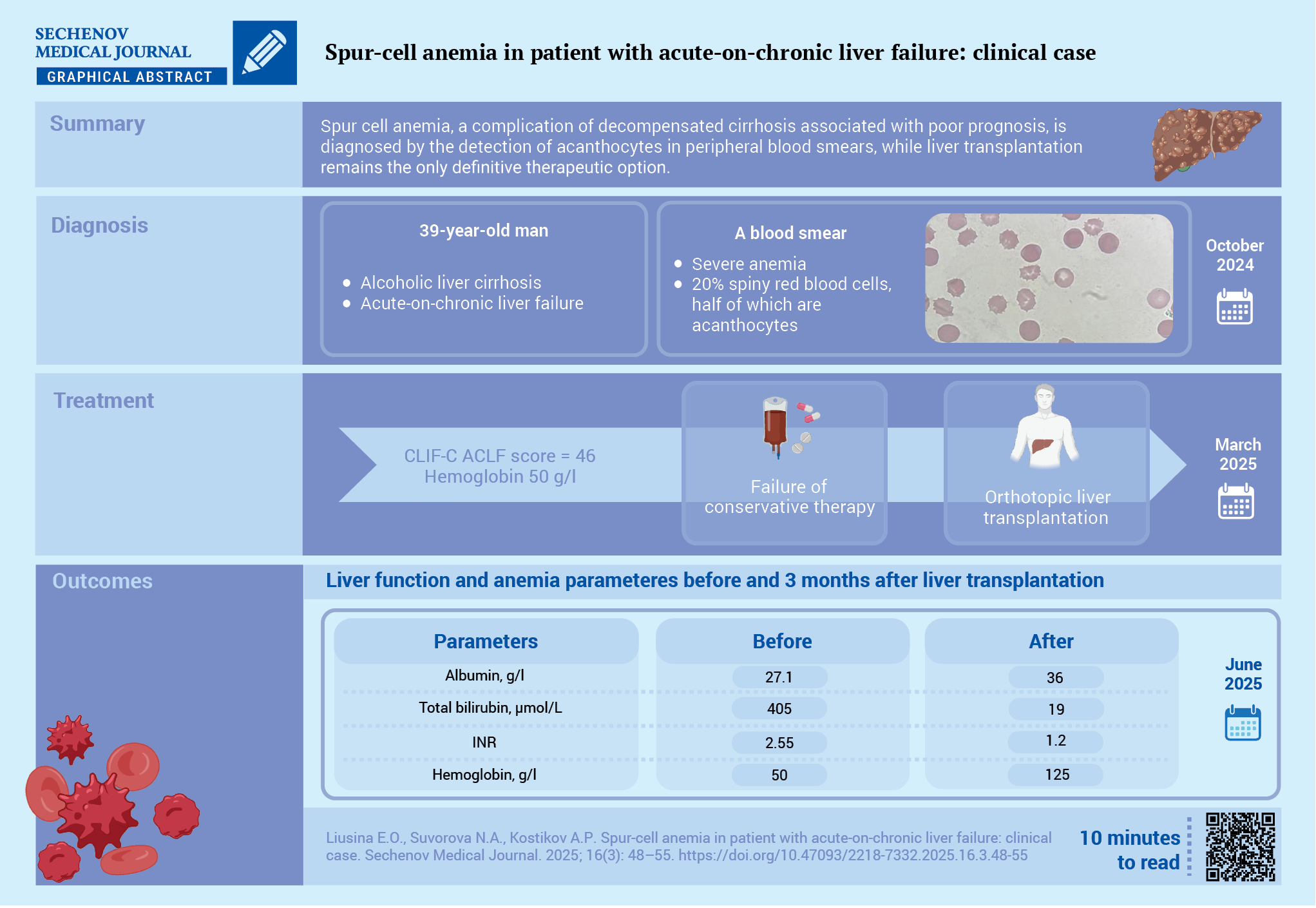
One of the rare forms of anemia in patients with liver cirrhosis (LC) is acanthocytosis (spur cell anemia) – a non‑immune hemolytic anemia caused by alterations in the lipid composition of the red blood cells membrane because of severe liver failure.
Case report. A 37‑year‑old patient with decompensated alcoholic LC (Child‑Pugh class C, the MELD‑Na (Model for End‑Stage Liver Disease – Na) score was 34 points) presented with severe weakness and dyspnea. Acute‑on‑chronic liver failure was diagnosed: CLIF‑C ACLF (Chronic Liver Failure Consortium Acute‑on‑Chronic Liver Failure Score) score was 46. Severe macrocytic anemia with reticulocytosis was detected: hemoglobin – 50 g/L, red blood cells – 1.26×10¹²/L, reticulocytes – 77.9 ‰. Other causes of anemia, such as blood loss, iron deficiency, vitamin B12 and folate deficiencies were excluded. The Coombs test was negative, and bone marrow examination ruled out myelodysplasia. Blood smear analysis revealed that 20% of red blood cells had the shape of spur cells, with approximately half of them being acanthocytes. Orthotopic liver transplantation was performed. Follow-up examination after three months showed normalization of liver function tests and absence of anemia and acanthocytosis.
Discussion. This case report highlights the need for blood smear examination to detect acanthocytes – a rare but prognostically unfavorable cause of anemia in patients with LC. Liver transplantation remains the only effective treatment option.

ISSN 2658-3348 (Online)

































