



Contents
Scroll to:
 K. Yu. Zherebchikova,
E. V. Poddubskaya,
A. P. Bondarenko,
A. A. Vilenskiy,
Yu. P. Sych,
V. V. Fadeev
K. Yu. Zherebchikova,
E. V. Poddubskaya,
A. P. Bondarenko,
A. A. Vilenskiy,
Yu. P. Sych,
V. V. Fadeev https://doi.org/10.47093/2218-7332.2026.17.1.1365
Scroll to:
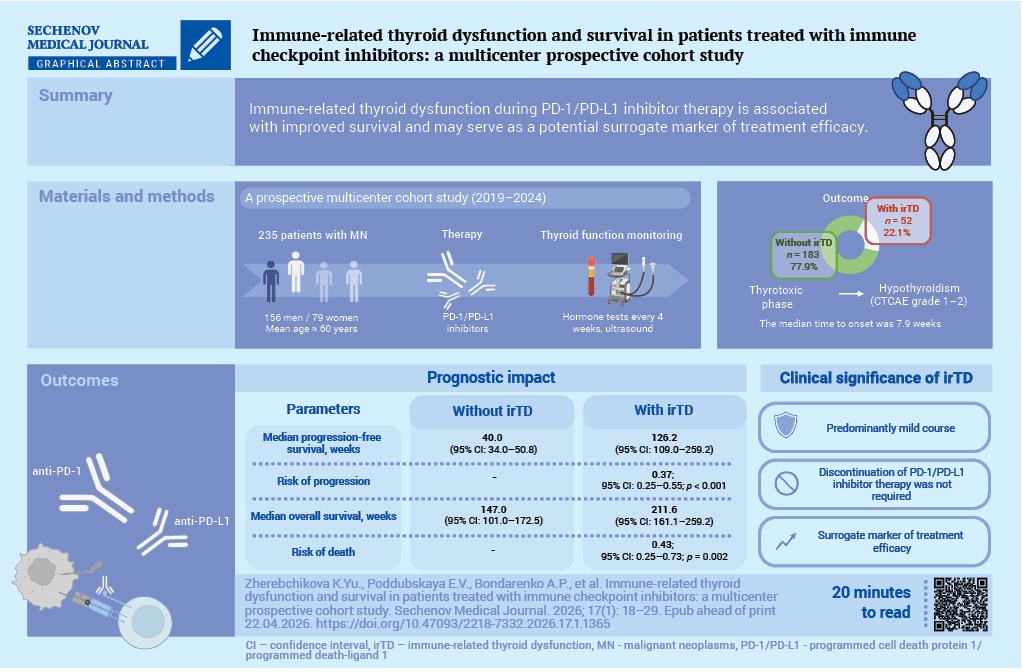
Aim. To assess the association between immune-related thyroid dysfunction (irTD) and overall survival or progressionfree survival in patients with malignant neoplasms receiving immune checkpoint inhibitor therapy.
Materials and methods. This multicenter prospective cohort study comprised 235 patients (156 men; mean age approximately 60 years) with histologically or cytologically confirmed malignancies of various localizations who were treated with programmed cell death protein 1/programmed death-ligand 1 (PD-1/PD-L1) inhibitors. Thyroid function was assessed before the treatment and every 4 weeks thereafter. irTD was diagnosed based on standardized biochemical and ultrasound criteria. Adverse events were graded according to CTCAE (Common Terminology Criteria for Adverse Events). Survival was analyzed using the Kaplan–Meier method, with comparisons performed using the log-rank test, and univariable Cox proportional hazards models, with hazard ratios (HRs) and 95% confidence intervals (CIs), were applied.
Results. irTD occurred in 52 patients (22.1%). In all cases, destructive thyroiditis with a transient thyrotoxic phase followed by hypothyroidism (CTCAE grade 1–2) was observed and did not require discontinuation of immune checkpoint inhibitors. The median time to irTD onset was 7.9 weeks. Patients with and without irTD were comparable in terms of sex, age, disease stage, previous cancer therapy, and type of PD-1/PD-L1 inhibitors. The development of irTD was associated with better progression-free survival (median 126.2 vs 40.0 weeks; HR 0.37; 95% CI: 0.25–0.55; p < 0.001) and better overall survival (211.6 vs 147.0 weeks; HR 0.43; 95% CI: 0.25–0.73; p = 0.002).
Conclusion. In this prospective multicenter cohort study, irTD occurred in approximately one-fifth of patients treated with PD-1/PD-L1 inhibitors, mainly during the first weeks of therapy, was generally mild, and was associated with improved survival. These findings suggest that irTD may be considered as a potential surrogate marker of treatment efficacy and support the need for regular monitoring of thyroid function during immunotherapy.
Malignant neoplasms remain one of the leading medical and social challenges worldwide, ranking among the top causes of morbidity, disability, and mortality. According to the International Agency for Research on Cancer (IARC), approximately 20 million new cases of malignant neoplasms (MN) and more than 9.7 million cancer-related deaths were recorded globally in 2022 [1]. It is projected that by 2050, the number of newly diagnosed cases may exceed 35 million, largely due to population aging, lifestyle changes, and exposure to environmental carcinogens [2].
A breakthrough in the systemic treatment of malignant neoplasms has been achieved with the introduction of immune checkpoint inhibitors (ICIs). Unlike cytotoxic and targeted therapies, these agents do not directly affect tumor cells but instead restore the ability of the immune system to recognize and eliminate them. Monoclonal antibodies targeting programmed cell death protein 1 (PD-1) and its ligand, programmed death-ligand 1 (PD-L1), have demonstrated substantial efficacy across a wide range of MN, including both localized and metastatic disease, significantly improving patient survival outcomes [1][3–5].
However, by enhancing immune activation, ICIs may also induce immune-related adverse events (irAEs) affecting various organs and systems. Thyroid dysfunction represents one of the most common irAEs associated with cancer immunotherapy [6]. The most frequent immune-related thyroid dysfunction (irTD) is destructive thyroiditis, typically characterized by an initial thyrotoxic phase followed by the development of persistent hypothyroidism requiring long-term hormone replacement therapy [7–9]. The pathogenesis of this complication remains incompletely understood; proposed mechanisms include immune-mediated destruction of thyroid follicular cells, activation of thyroid-specific autoantibodies, and cross-reactivity between tumor antigens and thyroid tissue [10][11].
Recent studies suggest that the development of irAEs, including thyroid dysfunction, may be associated with improved clinical outcomes in patients receiving ICI therapy [12–14].
The objective of this study was to evaluate the association between the development of irTD and overall survival as well as progression-free survival in patients with malignant neoplasms of various localizations treated with ICIs.
A multicenter prospective cohort observational study was conducted. Consecutive patients referred for scheduled systemic anticancer therapy for solid MN were enrolled at the following institutions: Sechenov First Moscow State Medical University (Sechenov University), Clinical Hospital of MEDSI Group JSC, University Clinic of Lomonosov Moscow State University, and multidisciplinary medical center VitaMed LLC. Patient recruitment was carried out between October 7, 2019, and December 27, 2024.
The sample size (n = 235) was determined at the study planning stage. It was based on the expected incidence of irTD of approximately 20–25%, according to published data on PD-1/PD-L1 inhibitor therapy, with an acceptable precision of the estimate (95% margin of error of approximately ± (5–6) percentage points). In addition, the planned sample provided a sufficient number of events for survival analysis: with 91 events, the study had 80% power to detect a moderate effect size (hazard ratio of approximately 0.5) at a two-sided significance level of 0.05.
The patient inclusion flowchart is presented in Figure 1. A total of 258 patients were screened for eligibility.
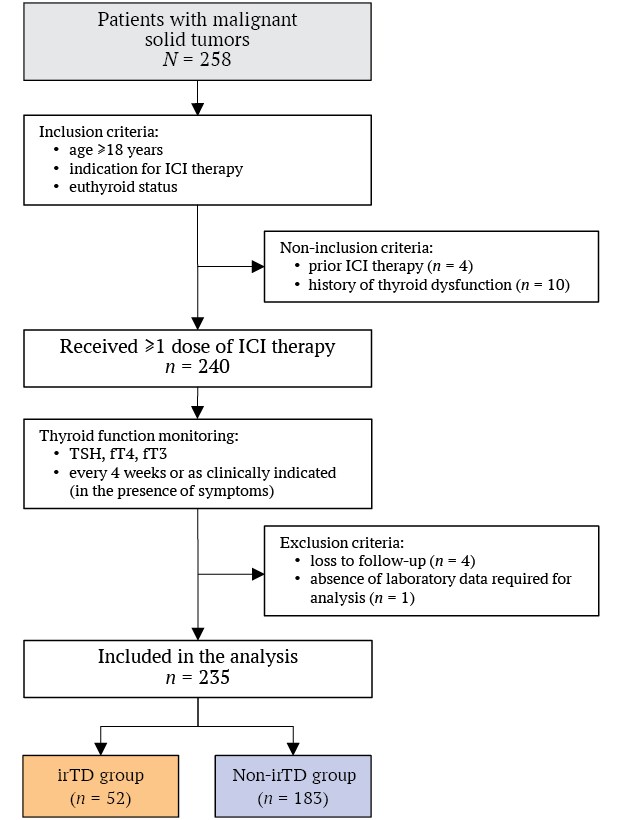
FIG. 1. Patient enrollment flowchart.
Note: fT3 – free triiodothyronine; fT4 – free thyroxine; ICI – immune checkpoint inhibitor; irTD – immune-related thyroid dysfunction; TSH – thyroid-stimulating hormone.
Inclusion criteria:
A total of 254 patients met the inclusion criteria.
Non-inclusion criteria:
Exclusion criteria:
Non-inclusion criteria were identified in 14 patients. Five patients were excluded from the final analysis: four due to loss to follow-up and one because of missing laboratory data. A total of 235 patients (156 men and 79 women) who received PD-1/PD-L1 inhibitor therapy for the first time were included in the study.
MN staging was performed according to the 8th edition of the TNM Classification of the American Joint Committee on Cancer (AJCC), applicable during the study period [15].
Thyroid hormone levels were assessed at baseline, as part of mandatory toxicity screening every 4 weeks after initiation of ICI therapy, and additionally whenever clinical symptoms suggestive of thyroid dysfunction occurred. Laboratory testing was centralized and performed at the independent laboratory INVITRO LLC. Serum thyroid-stimulating hormone (TSH), free thyroxine (fT4), and free triiodothyronine (fT3) concentrations were measured using a chemiluminescent immunoassay on the automated Alinity i analyzer (Abbott, USA) with manufacturer-provided reagents. Reference ranges were as follows: TSH, 0.4–4.0 µIU/mL; fT4, 9.0–19.05 pmol/L; fT3, 3.0–5.6 pmol/L.
Thyroid ultrasound was performed centrally at University Clinical Hospital No. 2 of I.M. Sechenov First Moscow State Medical University (Sechenov University) using a Voluson-i ultrasound system (General Electric, USA) with a 12-MHz linear transducer.
Hypothyroidism was diagnosed when TSH exceeded 4.0 µIU/mL in combination with normal or decreased fT4 levels.
Thyroiditis was diagnosed in the thyrotoxic phase when TSH was decreased with elevated or normal fT4 and/or fT3 levels, and in the hypothyroid phase when TSH was elevated with decreased or normal fT4 and/or fT3 levels1.
According to the recommendations of the National Comprehensive Cancer Network, destructive thyrotoxicosis was presumed when transient thyrotoxicosis spontaneously progressed to hypothyroidism during follow-up thyroid function assessment [16]. To exclude Graves’ disease, the absence of a characteristic clinical presentation (including orbitopathy), the absence of increased intrathyroidal vascularity on color Doppler ultrasonography, and the absence of increased blood flow velocity in the inferior thyroid artery >40 cm/s were additionally taken into account.
Progression-free survival was defined as the interval from initiation of ICI therapy to disease progression according to RECIST (Response Evaluation Criteria in Solid Tumors) version 1.1 criteria [17] or death from any cause, whichever occurred first. Overall survival was defined as the interval from initiation of ICI therapy to death from any cause or the date of last patient contact (censored observation). Tumor response assessment using computed tomography (CT) was performed every 12 weeks.
The severity of irAEs was graded according to the Common Terminology Criteria for Adverse Events (CTCAE) [18]. Follow-up was terminated upon progression of MN, death, or patient withdrawal from the study.
Continuous variables were assessed for normality using the Kolmogorov–Smirnov test. Variables with a normal distribution are presented as mean and standard deviation, whereas non-normally distributed variables are presented as median and interquartile range (25th–75th percentiles).
Categorical variables are reported as absolute counts and percentages. Comparisons between two groups for continuous variables with normal distribution and homogeneity of variances were performed using Student’s t-test. When the distribution deviated from normality, the nonparametric Mann–Whitney U test was applied.
Categorical variables were compared using Pearson’s chi-square test when expected frequencies exceeded 10; otherwise, the two-sided Fisher’s exact test was used. Survival analysis was performed using the Kaplan–Meier method. Differences between groups in time to death and disease progression were assessed using the log-rank test. Event risk was evaluated using univariable Cox proportional hazards models with calculation of hazard ratios (HRs) and 95% confidence intervals (CIs). A two-sided p value <0.05 was considered statistically significant.
Statistical analyses were performed using R software version 4.5.1 (R Foundation for Statistical Computing, Vienna, Austria) and StatTech version 4.6.1 (StatTech LLC, Russia).
During the entire follow-up period, irTD was identified in 52 patients (22.1%). At initial presentation, thyrotoxicosis and hypothyroidism occurred with equal frequency (26 cases each). Graves’ disease was excluded in all cases of thyrotoxicosis.
In all cases, thyrotoxicosis was transient and attributable to destructive thyroiditis. In one patient, hypothyroidism developed as part of autoimmune polyglandular syndrome, in combination with primary adrenal insufficiency and diabetes mellitus. The median time to onset of immune-related thyroid dysfunction from initiation of ICI therapy was 7.9 (6.0–9.1) weeks.
All patients with hypothyroidism received levothyroxine replacement therapy at doses of 75–150 µg/day, resulting in achievement and maintenance of TSH levels within the reference range. During the thyrotoxic phase of destructive thyroiditis, nine patients received beta-blockers for tachycardia control.
All thyroid dysfunction events were classified as grade 1 or 2 adverse events according to CTCAE and did not require treatment discontinuation or dose modification of ICI therapy.
In both groups, the majority of patients were men, with a mean age of approximately 60 years, and no significant differences were observed in these parameters. In nearly half of the patients in both groups, the primary tumor site was the lung (42–50%). Gastrointestinal malignancies (esophageal, gastric, and hepatic cancers) were observed in approximately 19–25% of patients, while cutaneous melanoma accounted for 12–19%. More than half of the patients had stage IV MN (Table).
Table. Baseline characteristics of patients with and without immune-related thyroid dysfunction
|
Variable |
irTD group (n = 52) |
Non-irTD group (n = 183) |
p value |
|
Male / female |
30 / 22 (57.7 / 42.3) |
126 / 57 (68.9 / 31.1) |
0.181 |
|
Age, years |
60.1 ± 12.0 |
60.5 ± 11.5 |
0.886 |
|
Primary tumor site |
|||
|
lung |
22 (42.3) |
92 (50.3) |
0.220 |
|
gastrointestinal tract |
13 (25.0) |
34 (18.6) |
|
|
melanoma |
10 (19.3) |
22 (12.0) |
|
|
other |
7 (13.5) |
35 (19.1) |
|
|
Tumor stage |
|||
|
I |
1 (1.9) |
7 (3.8) |
0.722 |
|
II |
9 (17.3) |
25 (13.7) |
|
|
III |
13 (25.0) |
35 (19.1) |
|
|
IV |
29 (55.8) |
116 (63.4) |
|
|
Previous treatment |
|||
|
systemic anticancer therapy |
28 (53.9) |
120 (65.6) |
0.055 |
|
surgery |
26 (50.0) |
73 (39.9) |
0.253 |
|
radiotherapy |
15 (28.9) |
46 (25.1) |
0.719 |
|
PD-1/PD-L1 inhibitors |
|||
|
nivolumab |
27 (51.9) |
98 (53.4) |
0.901 |
|
pembrolizumab |
17 (32.7) |
52 (28.4) |
|
|
tislelizumab |
3 (5.8) |
17 (9.3) |
|
|
atezolizumab |
3 (5.8) |
8 (4.4) |
|
|
avelumab |
2 (3.9) |
8 (4.4) |
Notes: quantitative variables are presented as mean with standard deviation (M ± SD), categorical variables are presented as the absolute number of patients with the characteristic and the proportion within the group, expressed as a percentage (in parentheses).
irTD – immune-related thyroid dysfunction; PD-1/PD-L1 – programmed cell death protein 1/programmed death-ligand 1.
No between-group differences were found regarding prior treatment history. A substantial proportion of patients in both groups had previously received systemic anticancer therapy (54–66%). Prior surgery had been performed in half of the patients in the first group and in 40% of those in the second group. Previous radiotherapy was reported in approximately one quarter of patients in both groups.
Most patients in both groups received PD-1 inhibitors. The most frequently prescribed agent was nivolumab, followed by pembrolizumab, whereas tislelizumab was used less often. The proportion of patients treated with PD-L1 inhibitors (atezolizumab or avelumab) was considerably lower, accounting for approximately 9–10% in each group.
Comparative analysis demonstrated that the development of irTD was significantly associated with a lower risk of disease progression compared with patients without thyroid dysfunction. The median progression-free survival in patients without thyroid dysfunction was 40.0 weeks from treatment initiation (95% CI: 34.0–50.8), whereas in patients who developed thyroid dysfunction it was 126.2 weeks (95% CI: 109.0–259.2).
In the univariable Cox proportional hazards model, the presence of irTD was associated with a statistically significant reduction in the risk of disease progression (HR 0.37; 95% CI: 0.25–0.55; p < 0.001), corresponding to an approximately 2.7-fold lower relative risk of the event (Fig. 2).
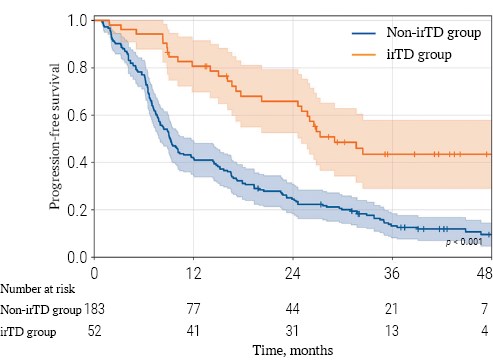
FIG. 2. Kaplan–Meier curve for progression-free survival.
Note: irTD – immune-related thyroid dysfunction.
By the end of follow-up, 91 deaths (38.7%) had been recorded. Comparative analysis demonstrated a statistically significant association between the development of irTD and a lower risk of death.
The median overall survival in patients without thyroid dysfunction was 147.0 weeks from treatment initiation (95% CI: 101.0–172.5), whereas in patients who developed thyroid dysfunction it was 211.6 weeks (95% CI: 161.1–259.2).
In the univariable Cox proportional hazards model, the development of irTD was associated with a statistically significant reduction in the risk of death (HR 0.43; 95% CI: 0.25–0.73; p = 0.002), corresponding to an approximately 2.3-fold lower relative risk of the event.
The 1-year and 3-year overall survival rates in the irTD group were 91.9% (95% CI: 79.9–96.9) and 69.9% (95% CI: 52.4–82.0), respectively, whereas in patients without thyroid dysfunction they were 69.0% (95% CI: 60.6–76.0) and 43.9% (95% CI: 33.3–53.9), respectively (log-rank test, p = 0.002; Fig. 3).
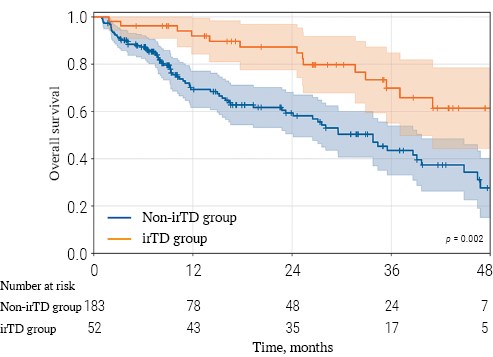
FIG. 3. Kaplan–Meier curve for overall survival.
Note: irTD – immune-related thyroid dysfunction.
The present study, which is the first prospective multicenter study conducted in the Russian Federation, demonstrated an association between the development of irTD and improved overall survival as well as progression-free survival in patients with various MN receiving PD-1/PD-L1 inhibitor therapy.
Our findings are consistent with the meta-analysis by Y.M. Cheung et al. [19], in which thyroid irAEs during ICI therapy were associated with an approximately 48% lower risk of death and a 42% lower risk of disease progression. In our cohort, the association with progression-free survival was even more pronounced: the presence of irTD was associated with a threefold increase in median progression-free survival and a 63% reduction in the risk of progression in the univariable Cox model. In addition, 1-year and 3-year overall survival in patients with thyroid dysfunction exceeded the corresponding values in patients without thyroid dysfunction by 22.9 and 26 percentage points, respectively.
It should be emphasized that our study included a heterogeneous population with different MN. In both groups, the lung was the most common primary tumor site, accounting for nearly half of all cases, followed by gastrointestinal malignancies (gastric, esophageal, and hepatic cancers), and cutaneous melanoma. Studies by Š. Cerić et al. [13], M. Xiao et al. [20], and A. Dawidowska et al. [14] in separate cohorts of patients with non-small cell lung cancer, gastric cancer, and melanoma, as well as several studies including mixed cancer populations [21][22], have shown that the development of irAEs, including thyroid events, is associated with improved efficacy of ICI therapy and better survival outcomes. In several studies, Cox models with time-dependent covariates treating thyroid dysfunction as an event occurring during follow-up were used to minimize immortal time bias and confirmed the robustness of this association [13][23].
Taken together, these findings support the notion that the association observed in the present study is reproducible across different patient populations, including both homogeneous disease-specific cohorts and heterogeneous cancer populations. Collectively, these data suggest that thyroid irAEs may serve as a potential surrogate marker of PD-1/PD-L1 inhibitor efficacy in patients with different MN. Although the exact biological mechanisms underlying this association remain under discussion, it has been proposed that the development of thyroid dysfunction reflects systemic immune activation induced by ICI therapy. In this context, thyroid dysfunction should not be viewed as an independent factor improving survival, but rather as a clinical marker of a more pronounced antitumor immune response, which may explain its association with more favorable oncologic outcomes [24][25].
Immune checkpoint inhibitors are believed to disrupt mechanisms of peripheral immune tolerance, leading to activation of autoreactive T-cell clones, T-cell-mediated injury of thyroid follicular epithelium, and the development of destructive thyroiditis. The serological profile of ICI-associated thyroid dysfunction differs from that of classical Hashimoto thyroiditis: thyroid autoantibodies are detected less frequently and usually at lower titers, suggesting only partial overlap of the immunopathogenesis with spontaneous autoimmune thyroid disease [24][26].
In our cohort, the overall incidence of irTD was 22.1%, which is comparable to the meta-analysis by J. de Filette et al. [10], where thyroid dysfunction was reported in approximately 20–30% of patients receiving PD-1/PD-L1 inhibitors. Thyroiditis most commonly developed within the first 8 weeks after initiation of ICI therapy, in agreement with previous studies by E.M. Presotto et al. [27] and R.M. Ruggeri et al. [28], in which the mean time to onset of thyroid adverse events was approximately 6–10 weeks.
In our cohort, the frequencies of thyrotoxic and hypothyroid phases were comparable, reflecting the heterogeneous clinical course of ICI-related thyroiditis described by C.A. Muir et al. [26]. All cases of thyrotoxicosis were transient and did not require antithyroid drug therapy. The absence of Graves’ disease is consistent with observations by H.J. Lee et al. [29], and J.C. Osorio et al. [11], who reported this condition to be a very rare complication of PD-1/PD-L1 inhibitor therapy. All thyroid dysfunction events were classified as grade 1–2 according to CTCAE and required neither treatment discontinuation nor dose modification. This is in line with international data showing that thyroid irAEs are usually mild to moderate and rarely necessitate cessation of ICI therapy.
Survival analysis was performed in the pooled cohort without detailed stratification by individual tumor types; therefore, our findings do not reflect potential differences across specific malignancies. In addition, we deliberately did not apply more complex time-bias adjustment methods because, given the available number of events, such approaches could have resulted in unstable and difficult-to-interpret estimates.
Future studies should focus on individual MN types, include longer follow-up periods, and formally account for time-related biases. Another promising development is the integration of clinical, immunological, and molecular-genetic markers to develop prognostic models in which irTD is considered within the broader context of the overall immune response to therapy.
This prospective multicenter study demonstrated that the development of irTD in patients with MN of various localizations receiving ICI therapy is associated with improved progression-free survival and overall survival. irTD occurred in approximately one fifth of patients, predominantly during the first weeks of treatment, was generally mild in severity, and did not require discontinuation or modification of immunotherapy.
These findings support the concept of thyroid dysfunction as a potential clinical marker of a more pronounced antitumor immune response and underscore the importance of regular thyroid function monitoring during ICI therapy.
Kristina Yu. Zherebchikova conceived and designed the study. Kristina Yu. Zherebchikova, Alexey A. Vilenskiy, Alexey P. Bondarenko, and Elena V. Poddubskaya collected and processed the data. Kristina Yu. Zherebchikova compiled the electronic database, performed the statistical analysis and interpretation of the results, and drafted the manuscript. Yulia P. Sych and Valentin V. Fadeev supervised the study and critically revised the manuscript. All authors read and approved the final version of the manuscript.
Ethics statements. The study protocol was reviewed and approved by the Local Ethics Committee of Sechenov First Moscow State Medical University (Sechenov University) (protocol No. 03-19 dated February 13, 2019). In accordance with existing cooperation agreements between the institutions, the conduct of the study at the Clinical Hospital of JSC “MEDSI Group of Companies”, the Department of Antitumor Drug Therapy of the Lomonosov Moscow State University Medical Research and Educational Center, and the multidisciplinary medical center “VitaMed” was carried out on the basis of this ethical approval. All patients provided written informed consent to participate in the study.
Data availability. The data that support the findings of this study are available from the corresponding authors on reasonable request. Data and statistical methods used in the article were examined by a professional biostatistician on the Sechenov Medical Journal editorial staff.
Conflict of interest. The authors declare that there is no conflict of interests.
Financing. The study had no sponsorship (own resources).
Use of artificial intelligence. No artificial intelligence tools were used in the preparation of this manuscript.
1. Ministry of Health of the Russian Federation. Hypothyroidism: clinical guidelines. 2024. https://cr.minzdrav.gov.ru/view-cr/531_4 (access date: 05.08.2025).
1. Bray F., Laversanne M., Sung H., et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2024 May-Jun; 74(3): 229–263. https://doi.org/10.3322/caac.21834. Epub 2024 Apr 4. PMID: 38572751
2. Filho A.M., Laversanne M., Ferlay J., et al. The GLOBOCAN 2022 cancer estimates: data sources, methods, and a snapshot of the cancer burden worldwide. Int J Cancer. 2025 Apr; 156(7): 1336–1346. https://doi.org/10.1002/ijc.35278. Epub 2024 Dec 17. PMID: 39688499
3. Wolchok J.D., Chiarion-Sileni V., Gonzalez R., et al. Overall Survival with Combined Nivolumab and Ipilimumab in Advanced Melanoma. N Engl J Med. 2017 Oct; 377(14): 1345– 1356. https://doi.org/10.1056/NEJMoa1709684. Epub 2017 Sep 11. Erratum in: N Engl J Med. 2018 Nov; 379(22): 2185. PMID: 28889792
4. Borghaei H., Paz-Ares L., Horn L., et al. Nivolumab versus Docetaxel in Advanced Nonsquamous Non-Small-Cell Lung Cancer. N Engl J Med. 2015 Oct; 373(17): 1627–1639. https://doi.org/10.1056/NEJMoa1507643. Epub 2015 Sep 27. PMID: 26412456
5. Overman M.J., McDermott R., Leach J.L., et al. Nivolumab in patients with metastatic DNA mismatch repair-deficient or microsatellite instability-high colorectal cancer (CheckMate 142): an openlabel, multicentre, phase 2 study. Lancet Oncol. 2017 Sep; 18(9): 1182–1191. https://doi.org/10.1016/S1470-2045(17)30422-9. Epub 2017 Jul 19. Erratum in: Lancet Oncol. 2017 Sep; 18(9): 510. PMID: 28734759
6. Higham C.E., Olsson-Brown A., Carroll P., et al. Society for endocrinology endocrine emergency guidance: Acute management of the endocrine complications of checkpoint inhibitor therapy. Endocr Connect. 2018 Jul; 7(7): G1–G7. https://doi.org/10.1530/EC-18-0068. PMID: 29930025
7. Zherebchikova K.Yu., Soltakhanova M.O., Sych Yu.P., et al. Prevalence, risk factors and features of the course of thyroid dysfunction induced by immunotherapy for cancer. Farmateka. 2025; 32(2): 109–115. (In Russian). https://doi.org/10.18565/pharmateca.2025.2.109-115. EDN: NLMGAB
8. Mao X., Mao C., Liu J., et al. Immune checkpoint inhibitor-induced thyroiditis and its potential mechanisms. Front Endocrinol (Lausanne). 2025 Jun; 16: 1584675. https://doi.org/10.3389/fen-do.2025.1584675. PMID: 40535343
9. Gong W., Zheng E., Liu M., et al. Risk factors and outcomes of thyroid immune-related adverse events following PD-1/PD-L1 inhibitors treatment in a large tertiary Chinese center. BMC Endocr Disord. 2025 Jul; 25(1): 171. https://doi.org/10.1186/s12902-025-01986-1. PMID: 40660166
10. de Filette J., Andreescu C.E., Cools F., et al. A Systematic Review and Meta-Analysis of Endocrine-Related Adverse Events Associated with Immune Checkpoint Inhibitors. Horm Metab Res. 2019 Mar; 51(3): 145–156. https://doi.org/10.1055/a-0843-3366. Epub 2019 Mar 12. PMID: 30861560
11. Osorio J.C., Ni A., Chaft J.E., et al. Antibody-mediated thyroid dysfunction during T-cell checkpoint blockade in patients with non-small-cell lung cancer. Ann Oncol. 2017 Mar; 28(3): 583–589. https://doi.org/10.1093/annonc/mdw640. PMID: 27998967
12. Das S., Johnson D.B. Immune-related adverse events and antitumor efficacy of immune checkpoint inhibitors. J Immunother Cancer. 2019 Nov; 7(1): 306. https://doi.org/10.1186/s40425-019-0805-8. PMID: 31730012
13. Cerić Š., Cerić T., Sokolović E., et al. Impact of thyroid immunerelated adverse events on clinical outcomes in non-small cell lung cancer (NSCLC) patients treated with checkpoint inhibitor therapy: A single center study. Biomol Biomed. 2025 Mar; 26(1): 144–149. https://doi.org/10.17305/bb.2025.12321. PMID: 40154981
14. Dawidowska A., Jagodzinska-Mucha P., Koseła-Paterczyk H., et al. Immune-Related Thyroid Adverse Events Predict Response to PD-1 Blockade in Patients with Melanoma. Cancers (Basel). 2022 Feb; 14(5): 1248. https://doi.org/10.3390/cancers14051248. PMID: 35267557
15. Amin M.B., Greene F.L., Edge S.B., et al. The Eighth Edition AJCC Cancer Staging Manual: Continuing to build a bridge from a population-based to a more “personalized” approach to cancer staging. CA Cancer J Clin. 2017 Mar; 67(2): 93–99. https://doi.org/10.3322/caac.21388. Epub 2017 Jan 17. PMID: 28094848
16. Thompson J.A., Schneider B.J., Brahmer J., et al. NCCN Guidelines® Insights: Management of Immunotherapy-Related Toxicities, Version 2.2024. J Natl Compr Canc Netw. 2024 Nov; 22(9): 582–592. https://doi.org/10.6004/jnccn.2024.0057. PMID: 39536465
17. Eisenhauer E.A., Therasse P., Bogaerts J., et al. New response evaluation criteria in solid tumours: revised RECIST guideline (version 1.1). Eur J Cancer. 2009 Jan; 45(2): 228–247. https://doi.org/10.1016/j.ejca.2008.10.026. PMID: 19097774
18. Freites-Martinez A., Santana N., Arias-Santiago S., Viera A. Using the Common Terminology Criteria for Adverse Events (CTCAE – Version 5.0) to Evaluate the Severity of Adverse Events of Anticancer Therapies. Actas Dermosifiliogr (Engl Ed). 2021 Jan; 112(1): 90–92. English, Spanish. https://doi.org/10.1016/j.ad.2019.05.009. Epub 2020 Sep 3. PMID: 32891586
19. Cheung Y.M., Wang W., McGregor B., Hamnvik O.R. Associations between immune-related thyroid dysfunction and efficacy of immune checkpoint inhibitors: a systematic review and meta-analysis. Cancer Immunol Immunother. 2022 Aug; 71(8): 1795–1812. https://doi.org/10.1007/s00262-021-03128-7. Epub 2022 Jan 13. PMID: 35022907
20. Xiao M., Qian L.L., Zhao Q., et al. Changes in thyroid hormone levels indicate immunotherapy efficacy in gastric cancer. Oncol Lett. 2025 May; 30(1): 364. https://doi.org/10.3892/ol.2025.15110. PMID: 40469917
21. Petrelli F., Grizzi G., Ghidini M., et al. Immune-related Adverse Events and Survival in Solid Tumors Treated With Immune Checkpoint Inhibitors: A Systematic Review and Meta-Analysis. J Immunother. 2020 Jan; 43(1): 1–7. https://doi.org/10.1097/CJI.0000000000000300. PMID: 31574022
22. Maillet D., Corbaux P., Stelmes J.J., et al. Association between immune-related adverse events and long-term survival outcomes in patients treated with immune checkpoint inhibitors. Eur J Cancer. 2020 Jun; 132: 61–70. https://doi.org/10.1016/j.ejca.2020.03.017. Epub 2020 Apr 22. PMID: 32334337
23. Ishidoya M., Makiguchi T., Tanaka H., et al. Endocrine immune-related adverse event is a prognostic biomarker independent of lead-time bias. Lung Cancer. 2024 Jun; 192: 107790. https://doi.org/10.1016/j.lungcan.2024.107790. Epub 2024 Apr 9. PMID: 38696920
24. Singh N., Hocking A.M., Buckner J.H. Immune-related adverse events after immune check point inhibitors: Understanding the intersection with autoimmunity. Immunol Rev. 2023 Sep; 318(1): 81–88. https://doi.org/10.1111/imr.13247. Epub 2023 Jul 26. PMID: 37493210
25. Karaviti D., Kani E.R., Karaviti E., et al. Thyroid disorders induced by immune checkpoint inhibitors. Endocrine. 2024 Jul; 85(1): 67–79. https://doi.org/10.1007/s12020-024-03718-2. Epub 2024 Feb 12. PMID: 38345684
26. Muir C.A., Clifton-Bligh R.J., Long G.V., et al. Thyroid Immunerelated Adverse Events Following Immune Checkpoint Inhibitor Treatment. J Clin Endocrinol Metab. 2021 Aug; 106(9): e3704– e3713. https://doi.org/10.1210/clinem/dgab263. PMID: 33878162
27. Presotto E.M., Rastrelli G., Desideri I., et al. Endocrine toxicity in cancer patients treated with nivolumab or pembrolizumab: results of a large multicentre study. J Endocrinol Invest. 2020 Mar; 43(3): 337–345. https://doi.org/10.1007/s40618-019-01112-8. Epub 2019 Sep 21. PMID: 31542865
28. Ruggeri R.M., Spagnolo C.C., Alibrandi A., et al. Predictors of thyroid adverse events during cancer immunotherapy: a real-life experience at a single center. J Endocrinol Invest. 2023 Nov; 46(11): 2399–2409. https://doi.org/10.1007/s40618-023-02096-2. Epub 2023 Apr 20. PMID: 37076759
29. Lee H.J., Manavalan A., Stefan-Lifshitz M., et al. Permanent hypothyroidism following immune checkpoint inhibitors induced thyroiditis may be associated with improved survival: results of an exploratory study. Front Endocrinol (Lausanne). 2023 Apr; 14: 1169173. https://doi.org/10.3389/fendo.2023.1169173. PMID: 37168978
Kristina Yu. Zherebchikova - Assistant Professor, Department of Endocrinology and Metabolic Health.
8/2, Trubetskaya str., Moscow, 119048
Elena V. Poddubskaya - Cand. of Sci. (Medicine), senior researcher, Institute for Personalized Oncology.
8/2, Trubetskaya str., Moscow, 119048
Alexey P. Bondarenko - oncologist, Head of the Day Hospital, LLC “VitaMed”.
10, Seslavinskaya str., Moscow, 121309
Alexey А. Vilenskiy - oncologist, Head of the Department of Anticancer Drug Therapy.
1, Leninskiye Gory, Moscow, 119991
Yulia P. Sych - Cand. of Sci. (Medicine), Associate Professor, Department of Endocrinology and Metabolic Health.
8/2, Trubetskaya str., Moscow, 119048
Valentin V. Fadeev - Dr. of Sci. (Medicine), corresponding member of RAS, Professor, Department of Internal Medicine, Faculty of Fundamental Medicine.
1, Leninskiye Gory, Moscow, 119991

|
1. STROBE Statement | |
| Subject | ||
| Type | Исследовательские инструменты | |
Download
(249KB)
|
Indexing metadata ▾ | |
Sechenov Medical Journal. Editor's checklist for this article you can find here.
Название / Title | Иммуноопосредованные тиреопатии и выживаемость пациентов, получающих терапию ингибиторами контрольных точек иммунного ответа: многоцентровое проспективное когортное исследование/ Immune-related thyroid dysfunction and survival in patients treated with immune checkpoint inhibitors: a multicenter prospective cohort study |
Раздел / Section
| ВНУТРЕННИЕ БОЛЕЗНИ/ INTERNAL MEDICINE
|
Тип / Article | Оригинальная статья / Original article |
Номер / Number | 1365
|
Страна/территория / Country/Territory of origin | Россия / Russia |
Язык / Language | Русский / Russian Английский / English
|
Источник / Manuscript source | Инициативная рукопись / Unsolicited manuscript |
Дата поступления / Received | 15.10.2025
|
Тип рецензирования / Type ofpeer-review | Двойное слепое / Double blind |
Язык рецензирования / Peer-review language | Русский / Russian
|
РЕЦЕНЗЕНТ А / REVIEWER A
Инициалы / Initials | 1365_А
|
Научная степень / Scientific degree | Кандидат медицинских наук / Cand. of Sci. (Medicine)
|
Страна/территория / Country/Territory | Россия / Russia
|
Дата рецензирования / Date of peer-review | 12.02.2026 |
Число раундов рецензирования / Number of peer-review rounds | 2 |
Финальное решение / Final decision | принять к публикации / accept
|
ПЕРВЫЙ РАУНД РЕЦЕНЗИРОВАНИЯ / FIRST ROUND OF PEER-REVIEW
Сильные стороны исследования
Слабые стороны исследования
Представленная работа соответствует правилам этики проведения исследований: авторы указали на положительное заключение локального этического комитета с номером протокола, пациенты подписывали информационное согласие для включения в исследование
Научная терминология, в целом, соответствует принятой в рассматриваемой области знаний. Однако рекомендуется заменить следующие термины:
Литературные источники валидны, большая часть опубликована за последние 5–6 лет (2019–2025). Работа обладает высокой степенью целостности и внутренней согласованности.
Имеются следующие замечания:
ЗАКЛЮЧЕНИЕ: переработка и повторное рецензирование.
ВТОРОЙ РАУНД РЕЦЕНЗИРОВАНИЯ
Авторы представили значительно переработанную версию рукописи, в которой были учтены практически все потенциальные замечания к оригинальной версии.
Рекомендации по незавершенным правкам:
ЗАКЛЮЧЕНИЕ: принять к публикации
РЕЦЕНЗЕНТ B / REVIEWER B
Инициалы / Initials | 1365_В
|
Научная степень / Scientific degree | Доктор медицинских наук / Dr. of Sci. (Medicine)
|
Страна/территория / Country/Territory | Россия / Russian
|
Дата рецензирования / Date of peer-review | 16.02.2026 |
Число раундов рецензирования / Number of peer-review rounds | 2 |
Финальное решение / Final decision | принять к публикации / accept
|
ПЕРВЫЙ РАУНД РЕЦЕНЗИРОВАНИЯ / FIRST ROUND OF PEER-REVIEW
В целом оценка статьи положительная, но требуется уточнить клиническое значение полученных результатов.
К серьезным ограничениям работы следует отнести отсутствие проведения мультифакторного анализа! Ведь развитие других серьезных НЯ (например, пульмонита) могло служить поводом для прекращения терапии ИКТИО. Возникновение гипотиреоза на фоне противоопухолевой терапии не требует ее прекращения, поэтому пациенты продолжали лечение.
Необходимо добавить информацию о развитии других НЯ в данной когорте. Сколько пациентов вынуждены были прекратить лечение? Среди пациентов, продолжавших и прекративших лечение, были различия по тиреоидной патологии? Если исследование было построено по принципу «intent to treat» (в рукописи обозначено, что был сплошной способ формирования выборки), то выбывание пациентов и прекращение лечения необходимо отразить в тексте статьи.
Если этот материал будет основой диссертационной работы, то лучше провести мультифакторный анализ. И в целом – смягчить формулировки (не повышает эффективность, а ассоциировано с лучшей выживаемостью). Статья может быть опубликована в журнале "Сеченовский вестник" после доработки.
ЗАКЛЮЧЕНИЕ: переработка и повторное рецензирование.
ВТОРОЙ РАУНД РЕЦЕНЗИРОВАНИЯ
Авторы внесли изменения в соответствии с замечаниями, возникшими при первом рецензировании статьи. Статья может быть принята к публикации
ЗАКЛЮЧЕНИЕ: принять к публикации
РЕКОМЕНДАЦИИ НАУЧНЫХ РЕДАКТОРОВ ЖУРНАЛА / RECOMMENDATIONS
OF THE SCIENTIFIC EDITORS OF THE JOURNAL
Этика
Указать дату этического одобрения и корректное название комитета.
Ключевые слова
Добавить 5–7 ключевых слов, слова не должны напрямую упоминаться в названии рукописи.
Ключевые положения
Добавить от 3 до 5 ключевых положений
Цель
Цель в аннотации и основном тексте должна совпадать.
Материалы и методы
Результаты
Технические требования

8-2 Trubetskaya st., Moscow, 119048
Federal State Autonomous Educational Institution of Нigher Education I.M.Sechenov First Moscow State Medical University of the Ministry of Health of the Russian Federation (Sechenovskiy University)
E-mail: sechenovmedj@staff.sechenov.ru
Processing of personal data
































