


INTERNAL MEDICINE

The literature review discusses approaches to the treatment of patients with chronic heart failure and preserved ejection fraction (EF>50) – HFpEF. The impact of various groups of drugs on the prognosis and quality of life of patients in this cohort was assessed based on the results of randomized trials, systematic reviews and meta-analyses, clinical recommendations of recent years. To date, only sodium-glucose cotransporter-2 inhibitors unequivocally improve the quality of life and prognosis of patients with HFpEF. Angiotensin receptor – neprilysin inhibitors and mineralocorticoid receptor antagonists are effective in terms of prognosis and quality of life only in patients with HFpEF in combination with resistant hypertension. In patients with sinus rhythm, heart rate > 70 beats/min and concomitant coronary artery disease, a combination of bisoprolol and ivabradine may be considered. Diuretics are recommended for patients with HFpEF when there are signs of congestion and signs of decompensation. Other groups of drugs do not significantly affect the quality of life and prognosis of patients with HFpEF and can be prescribed to such patients only as part of planned therapy for the treatment of other concomitant cardiovascular diseases.
The hepatobiliary system can be affected by a new coronavirus infection (COVID-19), in addition to the respiratory organs. Vanishing bile duct syndrome (VBDS) is a rare cause of jaundice that usually develops as a result of drug-induced liver injury or possibly due to the combined effect of several etiological factors.
Clinical case. A 77-year-old patient was hospitalized due to jaundice, skin itching and dark urine. Symptoms first appeared 1 month after COVID-19 treated with ceftriaxone and were accompanied by an increase in biochemical markers of cholestasis. Both extra- and intrahepatic bile ducts injuries were excluded. Liver histology revealed VBDS. Treatment with ursodeoxycholic acid for 11 months led to complete resolution of jaundice, regression of pruritus and a decrease in biochemical markers of cholestasis.
Discussion. This clinical case is of interest in connection with the development of VBDS in a patient after coronavirus pneumonia treated with ceftriaxone. VBDS is rarely included in the differential diagnosis of cholestatic syndrome, which is partly due to the lack of awareness of physicians about the complications that develop after COVID-19 and drug therapy.
COVID-19
Investigations into the causes of adverse outcomes of the novel coronavirus infection (COVID-19) have been ongoing since the beginning of the pandemic. There is evidence that coronavirus-induced cardiovascular injury is as important to a risk of adverse outcome as respiratory injury. Many studies have shown that concomitant cardiovascular disease aggravates the course of COVID-19. However, in some patients who did not have cardiovascular diseases before COVID-19, they are detected during hospitalization or after discharge from the hospital. The review examines data on the effect of serum biomarkers of cardiovascular disease determined during COVID-19 on the risk of adverse outcomes in the near and long-term follow-up periods. Among such biomarkers are considered: troponins, N-terminal pro B-type natriuretic peptide, creatine phosphokinase-MB, lactate dehydrogenase, myoglobin, growth stimulation expressed gene 2, pentraxin 3, angiotensin II, as well as D-dimer and homocysteine. Threshold values have been set for some of these biomarkers, which allow predicting the risk of an unfavorable outcome. At the same time, in most prognostic models, these markers are considered in association with cytokine storm indicators and other risk factors.
NEUROSURGERY
Aim. To identify predictors of surgical outcomes in patients with drug-resistant temporal lobe epilepsy in a multivariate model.
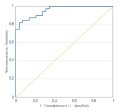
Materials and methods. Aretrospective study included 69 patients with drug-resistant temporal lobe epilepsy who underwent microsurgical anterior temporal lobectomy. The study included 31 (45%) men and 38 (55%) women. The median age was 28 (21; 36). Surgical treatment outcomes were assessed at 6, 12, 36, and 60 months after surgical intervention according to the Engel Epilepsy Surgery Outcome Scale. Logistic regression equations were calculated, a ROC curve was constructed, and odds ratio (OR) with 95% confidence interval (CI), sensitivity, specificity, area under the ROC curve (AUC) were calculated.
Results. In all assessed time periods, 88.3–93.0% of patients had outcomes consistent with Engel classes I and II. The distribution of patients by outcome classes did not change statistically significantly over the entire follow-up period. There were the following predictors of high efficacy of surgical treatment at 6 months after surgery: relatively shorter duration of active disease course (OR 0.719, 95%, CI: 0.437–0.966, p < 0.05), absence of status epilepticus (OR 0.048, 95% CI: 0.002–0.472, p < 0.05), absence of subdominant foci of irritative activity (OR 0.123, 95% CI: 0.012–0.845, p < 0.01), presence of mesial temporal sclerosis (OR 1008, 95% CI: 21.59–1310851, p < 0.01), a relatively longer resection margin on the temporal lobe (OR 637.32, 95% CI: 5.43–1960062, p < 0.05), lateralization of epileptogenic zone in subdominant hemisphere (OR 0.103, 95% CI 0.004–0.937, p = 0.0532). AUC was 0.957 (0.917–0.997), p < 0.0001; sensitivity 87.5%, and specificity 82.8%.
Conclusion. Independent predictors of the efficacy of microsurgical anterior temporal lobectomy in patients with drug-resistant temporal lobe epilepsy are the following: shorter duration of active disease course, absence of status epilepticus in the history, absence of subdominant foci, presence of mesial temporal sclerosis, a relatively longer resection margin on the temporal lobe, and lateralization of the epileptogenic zone in the temporal lobe of the subdominant hemisphere.
PATHOPHYSIOLOGY

Aim. To study the cytokine profile of the gingival crevicular fluid (GCF) in children with a juvenile rheumatoid arthritis (JRA).
Materials and methods. We examined 20 children with JRA and 10 patients without somatic pathology aged 6 to 16 years old. The condition of periodontal tissues was assessed by periodontal indices – gingival index GI (Loe, Silness, 1963) and gingival bleeding index GBI. Biomaterial sampling from the gingival sulcus was carried out using special endodontic absorbent paper points. Enzyme immunoassay for IL-18, IL-10, IL-1ß, IL-1RA, MCP-1, VEGFs in the GCF was performed using the test kits of Vector-Best LLC (Novosibirsk, Russia).
Results. Mean GI index in the JRA group was 0.31 ± 0.10 and in the control group – 0.20 ± 0.05 (p < 0.05), mean GBI index – 19.90 ± 3.14 and 10.80 ± 2.60 respectively (p < 0.05), which was accompanied by a more pronounced degree of inflammation of periodontal tissues. The GCF concentration of IL-18 in the JRA group was 6.70 (4.97–7.92) pg/ml, in the control group – 11.25 (8.70–13.10) pg/ml (p < 0.05), while the concentration of IL-1ß was 15.30 (13.79–17.18) pg/ml in the JRA group and 5.36 (5.32–5.54) pg/ml in the control group.
The IL-10 concentration in the JRA group was 3.60 (2.89–4.45) pg/ml, which was comparable to the values of the control group. The concentration of IL-1RA was lower in the JRA group than in the control group: 3638.5 (2397.5–4133.5) pg/ml and 4951.0 (4303.0–5455.0) pg/ml respectively. The total GCF chemokine concentration for MCP-1 was determined at the level of 15.65 (14.15–17.39) pg/ml and 15.50 (12.80–21.20) pg/ml for the main and control groups and for VEGF – 49.60 (41.95–54.50) pg/ml in the JRA group and 12.00 (11.00–13.00) pg/ml in control group.
Conclusion. In children with juvenile rheumatoid arthritis, an imbalance of pro- and anti-inflammatory cytokines in GCF plays a role in the development of gingivitis: an increased of IL-1ß concentration – a triggering factor of pro-inflammatory chains, a decreased concentration of IL-1RA – an anti-inflammatory cytokine, an increased concentration of VEGF – a marker of hypoxia.

ISSN 2658-3348 (Online)

































