


BIOMEDICAL STATISTICS TUTORIAL
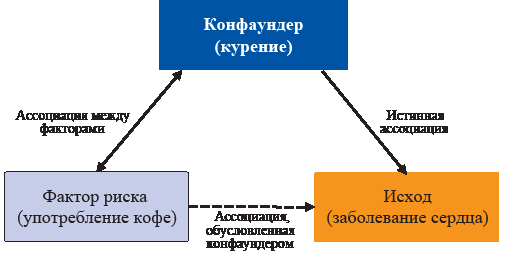
Adequate design is an essential condition for conducting a successful study. This review describes the most common types of research design in medicine. We discuss the differences between different types of observational and interventional studies, their advantages and limitations providing examples for each study design. The concept of bias and its potential sources in different studies are covered. We suggest the most suitable approaches to study design for different research objectives and outline approaches to data presentation. During the last decades, several guidelines for conducting and reporting different types of research were proposed and they are also covered in this manuscript.
SURGERY
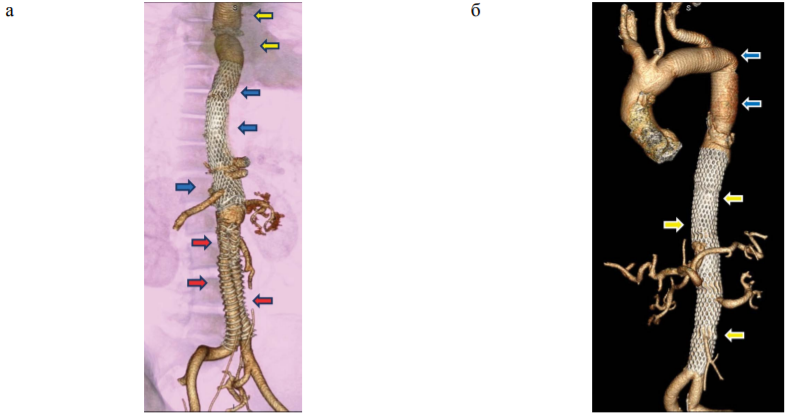
The aim. To evaluate the immediate outcomes after complete single-stage or step-by-step reconstruction of the primary and secondary distal aortic dissection using implantation of bare metal stents in the thoracoabdominal aorta.
Materials and methods. A prospective study was performed involving 21 patients (19 male) with aortic dissection: 8 had secondary distal dissection (group 1) and 13 had primary distal dissection (group 2). In all patients, indications for intervention were signs of malperfusion in one or more vascular regions. The following factors were evaluated: 30-day survival after surgery, causes of fatal outcomes, frequency and characteristics of non-fatal complications.
Results. The average age in group 1 was 43.0 ± 3.1 years, in group 2: 56.0 ± 3.9 years (p < 0.05). The most common cause of dissection in group 1 was connective tissue dysplasia, in group 2 – atherosclerosis in combination with arterial hypertension (p < 0.05). In group 1, 1 (13%) lethal outcome was registered, in group 2 – 4 (31%), the difference between the groups was not significant. Lethal complications were: multiple organ failure, stent implantation in the false aortic canal, aortic rupture, and thrombosis of the superior mesenteric artery. Non-fatal complications developed in group 1 in 3 (38%), in group 2 – in 3 (23%) patients, the difference between the groups is not significant. Among the non-lethal complications, malperfusion of the upper and lower extremities was diagnosed, requiring stent placement, prosthetics or bypass surgery; cerebrospinal circulation disorder, acute cerebrovascular accident, multiple organ failure, conservatively treated.
Conclusion. The survival rate for 30 days after a complete single-stage or step-by-step reconstruction of the primary and secondary distal aortic dissection using implantation of bare metal stents in the thoracoabdominal aorta is 76%, the frequency of non – fatal complications is 28%.
ONCOLOGY
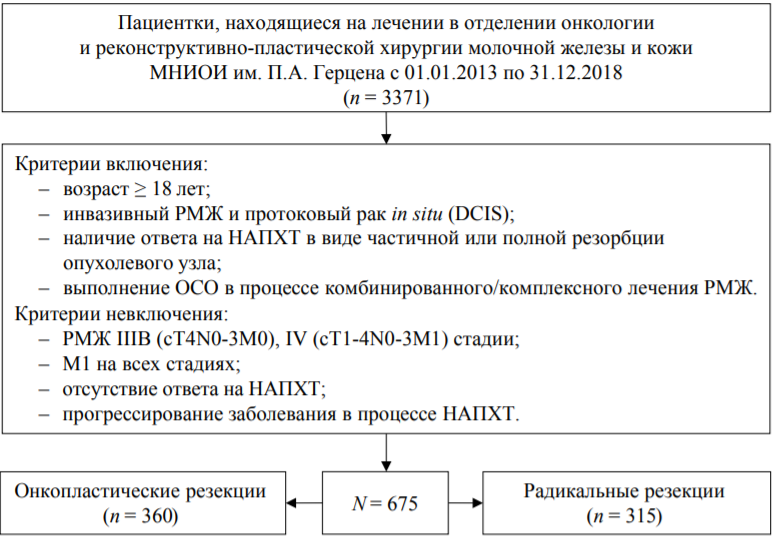
Aim. To determine the frequency of local recurrence of breast cancer (BC) after performing breast-conserving surgery (BCS) during and after complex treatment, to study the risk factors for local recurrence and survival.
Materials and methods. A retrospective cohort study of 675 patients with breast cancer who underwent BCS followed by remote radiotherapy was conducted. The frequency of local relapse and risk factors were studied, 3- and 5-year local-free survival. The odds ratios (OR) and 95% confidence intervals (CI) were calculated, and the Kaplan–Meyer curves were constructed.
Results. Radical breast resections (RBR) were performed in 46.7% of patients, and oncoplastic breast resections (OBS) in 53.3% of patients. The most common histological type in both groups was invasive cancer with no signs of specificity: 76.9% and 84.1% – in the OBS and RBR groups, respectively. The incidence of cancer in situ was higher in the OBS group: 14.7% vs. 3.3% in the RBR group (p < 0.001), metastases in regional lymph nodes were more frequent in the RBR group: 34.3% against 20.3% in OBS (p < 0.001). According to the immunohistochemical type and degree of differentiation, the groups did not differ. For 3 years, the relapse-free survival rate was 99.7% in both groups, and for 5 years – 99.2% in the OBS group. and 99.7% in the RBR group, 6 years – 98.3% and 98.7%, respectively; no significant differences were found between the groups. There were no statistically significant differences in the frequency of relapses depending on the width of the resection edges from <1 to ≥10 mm. The risk of relapse was increased with a preserved menstrual status (OR 20.05; 95% CI 2.52–159.33), Her2/neu–positive (OR 5.11; 95% CI 1.04–25.09) and triple-negative types (OR 4.02; 95% CI 1.02–15.95), the degree of differentiation of G3 (OR 5.58; 95% CI 1.59–19.64).
Conclusion. BCS is characterized by oncological safety; the rate of local relapse within 6 years is 1.5%. Risk factors for relapse include active menstrual status, highly aggressive immunohistochemical types of breast cancer, and low degree of differentiation.
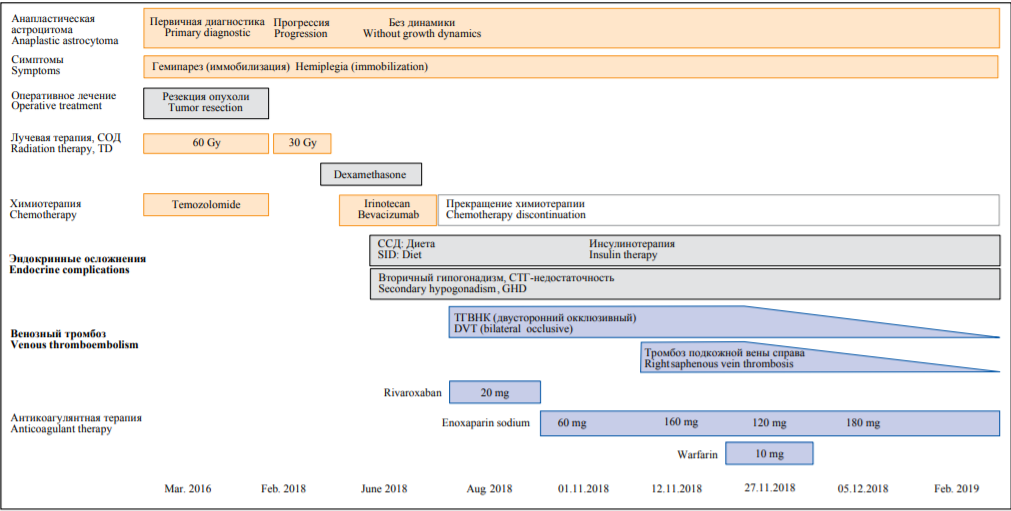
Venous thromboembolism occurs in 48–200 out of 1,000 patients with brain cancer per year, which is significantly more frequent than in general population.
Case report. A female patient had surgical treatment of anaplastic astrocytoma following radiotherapy and chemotherapy (temozolomide, irinotecan, bevacizumab) at the age of 17 years old. She also received dexamethasone. At the age of 20 years, she developed cancer recurrence, that required chemotherapy. After chemotherapy had been initiated, the patient developed deep vein thrombosis of the legs. Rivaroxaban 20 mg/d for 2.5 months with the subsequent switch to enoxaparin 60 mg/d showed no recanalization. Enoxaparin dose increasing up to 160 mg/d demonstrated incomplete recanalization, however, superficial venous thrombosis of the legs developed. Combination therapy with enoxaparin plus warfarin resulted in further deep and superficial veins recanalization.
Discussion. In cancer-associated venous thromboembolism that is resistant to low molecular weight heparin monotherapy, short-term combination therapy with low molecular weight heparin and vitamin K antagonists can be considered. However, in recurrent cancer standard treatment protocols can be ineffective.
INTERNAL MEDICINE
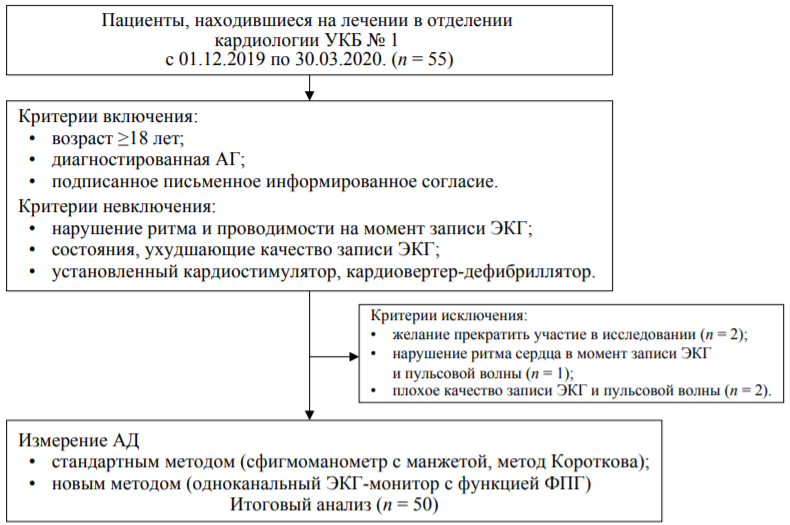
The aim. To evaluate the reliability of blood pressure (BP) measurement results using a cuffless blood pressure device (CardioQVARK®) in comparison with the values obtained using the Korotkov method.
Materials and methods. An observational cross-sectional study of 50 patients (25 men, mean age 60 ± 14 years) with arterial hypertension was performed. Blood pressure was measured by the Korotkov method as a standard method, and a CardioQVARK® device, made in the form of a smartphone case, was used as a new method. The device records the electrocardiogram and the photoplethysmogram. Based on the parameters of the electrocardiogram and the photoplethysmogram the systolic and diastolic blood pressure (SBP and DBP) is calculated. Correlation analysis, Student’s t-test, Bland-Altman method were used for comparing the two methods, the standard deviation of the difference and a 95% confidence interval (95% CI) were calculated.
Results. There were no statistically significant differences in the mean values of SBP and DBP for the two methods. There was a strong direct relationship between SBP (r = 0.976, p < 0.0001) and DBP (r = 0.817, p < 0.0001), measured by two methods. Bias for SBP and DBP measured by the new method was: –0.5 mm Hg (95% CI: –1.7; 0.7) and –0.3 mmHg (95% CI: –1.4; 0.7), respectively. The difference in DBP measurements depended on the blood pressure level (r = 0.302, p = 0.03). The underestimation of DBP values was more pronounced for low blood pressure from 55 to 75 mm Hg. At the time of the study, 13 (26%) patients had an increase in blood pressure. The sensitivity of the new method in detecting arterial hypertension was 77% (95% CI: 46; 95), specificity 100% (95% CI: 91; 100), accuracy 94% (95% CI: 83; 99).
Conclusion. The blood pressure measurement method based on the analysis of the electrocardiogram and photoplethysmogram showed reliable blood pressure measurement results in comparison with the Korotkov method.

The number of transplantation and transplant survival rates increase steadily. Patients after solid organ transplantation re-ceive lifelong immunosuppressive therapy which may have adverse effects on carbohydrate and lipid metabolism. The most diabetogenic drugs are calcineurin inhibitors and corticosteroids. Posttransplant diabetes mellitus (PTDM) is hyperglycemia that meets American Diabetes Association and World Health Organization diabetes criteria for nontransplant patients and that was newly diagnosed after transplantation. PTDM may worsen both short-term and long-term transplantation outcomes so that the problem of timely diagnosis, proper treatment and prevention is critical. In early post-transplant period, transient hyperglycemia is found in the vast majority of patients; therefore, PTDM screening is carried out at least one month after transplantation. The gold standard test for PTDM diagnosis is oral glucose tolerance test. In the same time diagnostic value of hemoglobin A1C is limited. Lifestyle therapy and antidiabetic drugs are considered as possible preventive measures. Stress induced hyperglycemia management in solid organ recipients is the same with other surgical patients. Which organ was transplanted, patient characteristics and possible drug interactions with immunosuppressive therapy should be taken into account while managing PTDM. Blood pressure and lipid profile should be under control for comprehensive cardiovascu-lar risk reduction. It remains unclear which PTDM treatment and prevention strategy is the best and for better understanding interdisciplinary approach is needed.
PATHOLOGICAL PHYSIOLOGY
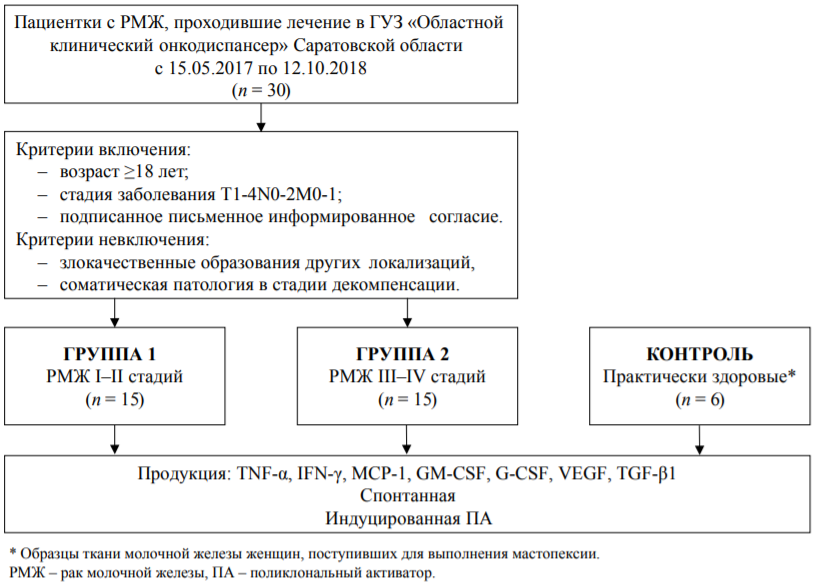
Aim. To study the spontaneous and stimulated production of cytokines in biopsies of breast cancer (BC) depending on the cancer stage.
Materials and methods. An experimental study was carried out with cell cultures of breast cancer biopsies of stages I–II (group 1, n = 15) and III–IV stages (group 2, n = 15). The control consisted of 6 healthy women who underwent mastopexy. We used enzyme immunoassay method to access spontaneous and induced by a complex of polyclonal activators (PA: phytohemagglutinin 4 μg / ml, concanavalin A 4 μg / ml, lipopolysaccharide 2 μg / ml) concentration of TNF-α, IFN-γ, G-CSF, GM-CSF, VEGF, MCP-1, TGF-β1. The index of the effect of polyclonal activators (IVPA) on cytokine production (induced production / spontaneous production) was calculated. To compare groups, the Mann-Whitney test and the median test, the chi-square test and the Fisher’s exact test were used.
Results. Groups 1 and 2 did not differ in age, histological variant and immunohistochemical type of tumour, predominantly invasive cancer without signs of specificity prevailed. In group 2, a pronounced vascularization was more often observed: in 6 (40%) patients versus 1 (7%) in group 1 (p < 0.05). In both groups, compared with the control, there was a statistically sig-nificant (p < 0.05) increase in spontaneous production of TNF-α by 4.2 and 4.8 times, MCP-1 by 6.7 and 6.3 times, TGF-β1 – 2.2 and 2.5 times, VEGF 11.9 and 14.6 times; GM-CSF 15.6 and 13.4 times, G-CSF 96.8 and 79.5 times, respectively. The concentration of MCP-1 and IFN-γ was higher in group 1 (p < 0.05), VEGF and TGF-β1 – in group 2 (p < 0.05). IVPA in group 2 exceeded similar values in group 1 for G-CSF, VEGF, TGF-β1 (p < 0.05).
Conclusion. The production of cytokines (TNF-α, MCP-1, GM-CSF, G-CSF, VEGF, TGF-β1) in breast cancer biopsies is significantly higher than in biopsies of the unchanged mammary gland and depends on the stage of the tumour process.
ERRATUM

ISSN 2658-3348 (Online)

































